All SubjectsAnatomy (9)Anesthesiology (4)Biochemistry (11)Community Medicine (13)Dermatology (4)ENT (3)Forensic Medicine (7)Internal Medicine (14)Microbiology (7)Obstetrics and Gynecology (15)Ophthalmology (3)Orthopaedics (4)Pathology (14)Pediatrics (7)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (6)
Q11
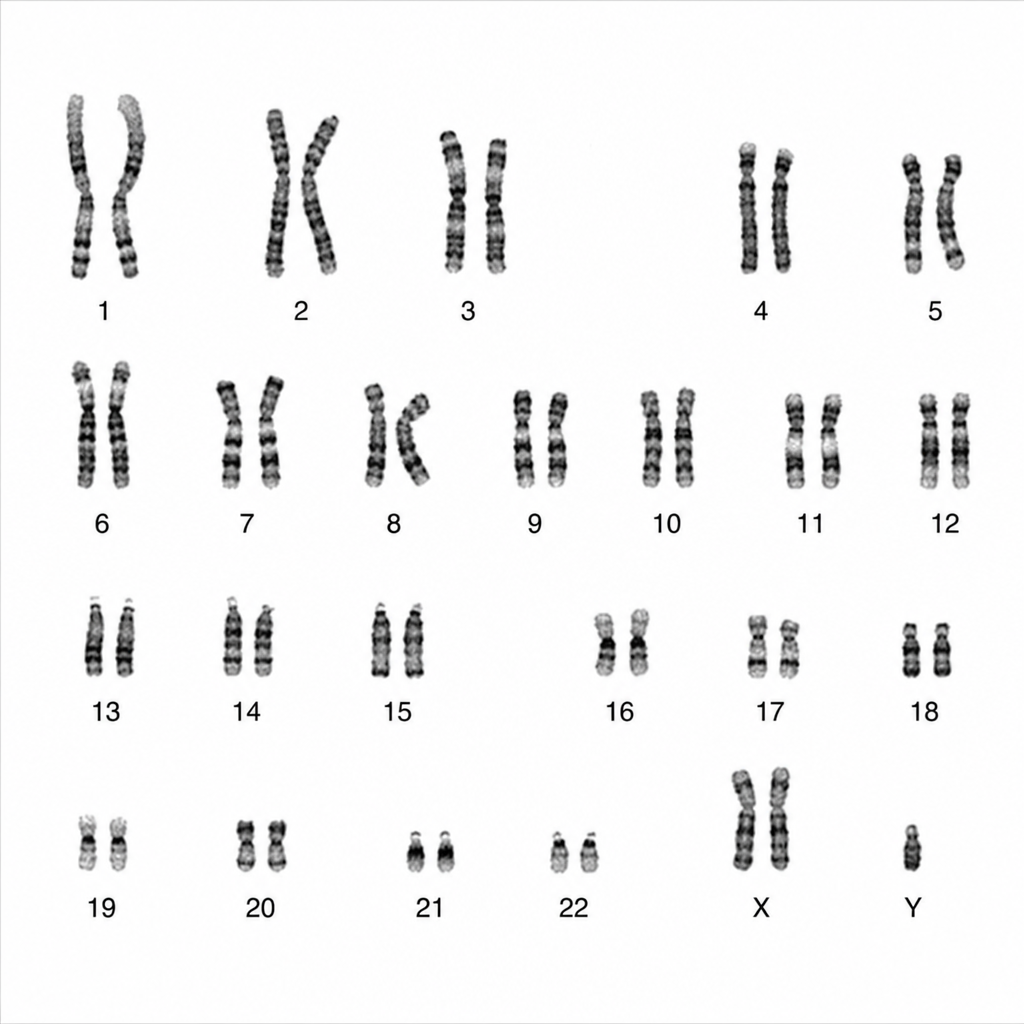
A karyotyping image is given below. What are the clinical features most likely to be expected in such patients?
Q12
Which of the following is not likely to be seen in a patient with Paroxysmal Nocturnal Hemoglobinuria (PNH)?
Q13
A 45-year-old male patient presented with a history of bilateral lower limb weakness, which progressed to his upper limbs in a year. On examination, he had weakness in both lower limbs and wasting in the left upper limb. Babinski sign was positive and the deep tendon reflexes were hyperactive. He has no sensory loss or any autonomic dysfunction. What is the likely diagnosis?
Q14
A 62-year-old male patient with heart failure is scheduled for a heart transplant. His renal function test is deranged, and haemoglobin is $6 \mathrm{gm} \%$. The physician ordered 2 units of whole blood. Four hours after transfusion, he developed severe respiratory distress. On examination, he is hypoxemic, has tachycardia and his mean arterial pressure is elevated. Which of the following are the best investigations for the above scenario? 1. Chest X-ray 2. Brain natriuretic peptide (BNP) level 3. Absolute neutrophil count 4. Leucocyte antibodies 5. Platelets