INI-CET 2021 — Community Medicine
12 Previous Year Questions with Answers & Explanations
SAFE strategy for trachoma includes all except?
Mobile Medical Units (MMUs) under government health programs can operate through different models. Which of the following statements about MMU operations are correct? 1. MMUs are run by the government 2. MMUs are run by external agencies with medical supplies given by the government 3. MMUs are run by the government and medical supplies are also given by the government 4. MMUs are run by external agencies and medical supplies are also given by the external agency
You are starting services for hypertension in your PHC. 50 patients who required antihypertensive treatment were transferred from another center. 40 of them were on amlodipine ( 5 mg PO) and 10 were on lisinopril ( 10 mg PO) as they had contraindications to the use of amlodipine. The drugs are supplied at the PHC on a monthly basis and you have to place an order for their medications. What is the number of tablets that you will order and the reorder factor?
Compared to a pregnant female, a lactating female would require a higher level of nutrient supplementation for which of the following?
The most common mode of absorption of inorganic lead in industries leading to lead poisoning is:
A nurse keeps the bins as shown in the image in the hospital ward. Which of the following items would go into the black bin?

Interpret the following graph.
Which of the following is not a part of case-control studies?
A new drug has been introduced into the market which was found to decrease mortality but it does not cure the disease. Which of the following is a true statement regarding prevalence and incidence?
What is triage for?
INI-CET 2021 - Community Medicine INI-CET Practice Questions and MCQs
Question 1: SAFE strategy for trachoma includes all except?
- A. Antibiotics
- B. Surgery for trichiasis
- C. Facial cleanliness
- D. Evaluation of control program (Correct Answer)
Explanation: ***Evaluation of control program*** - **Evaluation** is a monitoring and assessment process used to measure the effectiveness of the SAFE strategy, but it is **not one of the four intervention components** of the strategy itself. - The SAFE strategy consists of: **S**urgery, **A**ntibiotics, **F**acial cleanliness, and **E**nvironmental improvement. *Surgery for trichiasis* - **Trichiasis** (in-turned eyelashes) is a blinding complication of trachoma requiring **surgical correction** to prevent corneal damage. - This is the "S" component of SAFE. *Antibiotics* - **Mass drug administration** with **azithromycin** (single oral dose) is used to reduce the community reservoir of *Chlamydia trachomatis*. - This is the "A" component of SAFE. *Facial cleanliness* - Promoting **facial hygiene**, especially in children, prevents transmission of *Chlamydia trachomatis* through contact and fly vectors. - This is the "F" component of SAFE. *Environmental improvement (Not listed as an option but part of SAFE)* - Improving **water supply**, **sanitation**, and **waste management** reduces breeding sites for flies and improves hygiene. - This is the "E" component of SAFE.
Question 2: Mobile Medical Units (MMUs) under government health programs can operate through different models. Which of the following statements about MMU operations are correct? 1. MMUs are run by the government 2. MMUs are run by external agencies with medical supplies given by the government 3. MMUs are run by the government and medical supplies are also given by the government 4. MMUs are run by external agencies and medical supplies are also given by the external agency
- A. 1, 2, 3, and 4
- B. 1 and 2
- C. 1, 2, and 3 (Correct Answer)
- D. Only 1
Explanation: ***1, 2, and 3*** - This option correctly identifies the flexible operational models of **Mobile Medical Units (MMUs)** under government health programs. - MMUs can be directly managed by the **government**, managed by **external agencies** with government-provided supplies, or managed by the government with **government-provided supplies**. *1, 2, 3, and 4* - This option incorrectly includes the scenario where MMUs are run by **external agencies** and medical supplies are also provided by the **external agency**. - While external agencies can run MMUs, government health programs typically ensure that essential medical supplies are provided or funded by the **government** to maintain standardization and accessibility. *1 and 2* - This option is incomplete as it misses the model where both the MMU operation and medical supplies are provided by the **government** (statement 3). - Government health programs often have fully integrated models, especially in remote areas. *Only 1* - This option is too restrictive, as it only includes the model where MMUs are run by the **government**. - MMUs often involve partnerships with **external agencies** for operational efficiency or specialized services.
Question 3: You are starting services for hypertension in your PHC. 50 patients who required antihypertensive treatment were transferred from another center. 40 of them were on amlodipine ( 5 mg PO) and 10 were on lisinopril ( 10 mg PO) as they had contraindications to the use of amlodipine. The drugs are supplied at the PHC on a monthly basis and you have to place an order for their medications. What is the number of tablets that you will order and the reorder factor?
- A. 1000, rf=3
- B. 1600, rf=2 (Correct Answer)
- C. 1200, rf=2
- D. 1400, rf=3
Explanation: ***1600, rf=2*** - **Monthly requirement calculation:** 40 patients need amlodipine (40 × 30 = 1,200 tablets/month) and 10 patients need lisinopril (10 × 30 = 300 tablets/month), totaling **1,500 tablets per month**. - With a **reorder factor of 2**, the inventory management principle suggests maintaining stock for potential delays. Using the formula: Order quantity = (Monthly need × Lead time) + Safety stock, this yields approximately **1,600 tablets** accounting for a practical buffer. - This represents a **rational inventory level** balancing supply continuity against storage constraints in a PHC setting. *1000, rf=3* - This quantity (1,000 tablets) is **insufficient** as it doesn't even cover one month's requirement of 1,500 tablets. - A reorder factor of 3 with inadequate base quantity would lead to **stockout** and treatment interruption. *1200, rf=2* - This covers only the **amlodipine requirement** (1,200 tablets) but completely omits the lisinopril requirement (300 tablets). - Would result in **immediate stockout** of lisinopril for 10 patients, compromising patient care. - Does not account for any **safety stock** or lead time buffer. *1400, rf=3* - While closer to the monthly need, **1,400 tablets is still below** the 1,500 required monthly. - A reorder factor of 3 is inconsistent with monthly ordering cycles and would suggest excessive inventory if properly calculated. - Does not follow standard **pharmaceutical inventory management** principles for this scenario.
Question 4: Compared to a pregnant female, a lactating female would require a higher level of nutrient supplementation for which of the following?
- A. Calcium (Correct Answer)
- B. Folic acid
- C. Iron
- D. Vitamin A
Explanation: ***Calcium*** - **Lactating women** require higher calcium intake compared to pregnant women due to significant calcium transfer into **breast milk** for infant bone development. - This increased demand helps maintain maternal bone density and ensures adequate calcium supply for the baby. *Folic acid* - **Folic acid** is critically important during **pregnancy** to prevent neural tube defects, with supplementation typically decreasing postpartum. - While still necessary, the daily recommended intake for lactating women is generally lower than during pregnancy. *Iron* - **Iron requirements** are highest during **pregnancy** to support increased maternal blood volume and fetal development. - In lactating women, iron needs often decrease postpartum, especially if there was minimal blood loss during delivery and menstruation has not yet resumed. *Vitamin A* - While **Vitamin A** is important for both pregnant and lactating women, the recommended intake for pregnant women tends to be slightly higher, especially for **fetal organ development**. - Excessive vitamin A can be teratogenic during pregnancy, so supplementation needs careful monitoring in both states.
Question 5: The most common mode of absorption of inorganic lead in industries leading to lead poisoning is:
- A. Inhaled lead dust (Correct Answer)
- B. Ingestion of contaminated food and water
- C. Contaminated hands
- D. Absorption through skin
Explanation: ***Inhaled lead dust*** - In industrial settings, **inorganic lead** is frequently present as fine airborne particles, making inhalation the primary route of exposure and absorption. - **Lead dust** generated from processes like smelting, battery manufacturing, and construction (e.g., sanding lead paint) can be readily absorbed through the respiratory tract. *Ingestion of contaminated food and water* - While ingestion of **contaminated food and water** is a significant route of lead exposure, especially in children, it is generally less common than inhalation in occupational settings where lead dust is prevalent. - This route is more typically associated with environmental contamination rather than direct industrial absorption. *Contaminated hands* - **Contaminated hands** pose a risk primarily through transfer of lead to the mouth and subsequent ingestion, rather than direct absorption through the skin itself. - This is an indirect route of internal exposure, often secondary to handling lead-containing materials without proper hygiene. *Absorption through skin* - **Inorganic lead** (the type commonly found in industrial settings) is very poorly absorbed through intact skin. - **Organic lead compounds** (e.g., tetraethyl lead), which are less common in general industries, are much more readily absorbed cutaneously.
Question 6: A nurse keeps the bins as shown in the image in the hospital ward. Which of the following items would go into the black bin?
- A. Gloves
- B. Soiled linen bedsheet
- C. Contaminated gloves
- D. Glove paper cover (Correct Answer)
Explanation: ***Glove paper cover*** - The black bin is typically designated for **general waste** that is neither infectious nor sharp. - A glove paper cover is considered **non-hazardous**, non-recyclable waste and would be appropriately disposed of in a black bin. *Gloves* - **Used gloves**, even if not obviously contaminated with bodily fluids, are considered potentially infectious waste and should not be placed in the black bin. - These should generally be disposed of in a **yellow bag or bin** (infectious waste) to prevent cross-contamination. *Soiled linen bedsheet* - A soiled linen bedsheet is considered **infectious waste**, as it may contain bodily fluids or pathogens. - This type of waste requires specific handling and disposal, usually in **red bags or bins**, not general waste. *Contaminated gloves* - **Contaminated gloves** are classified as infectious waste and must be disposed of in designated containers for biohazard materials. - Placing them in a black bin would pose a **risk of infection** to waste handlers and is against standard medical waste disposal protocols.
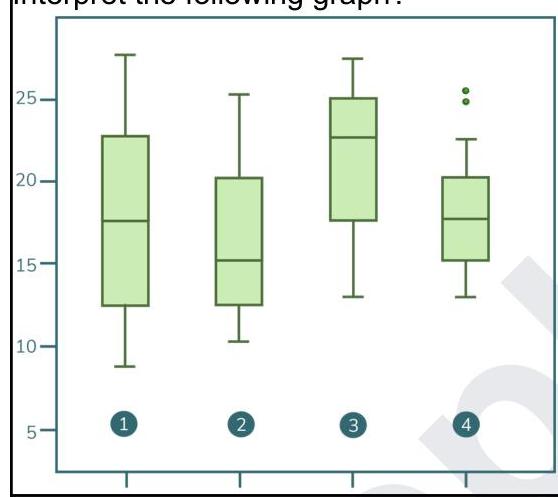
Question 7: Interpret the following graph.
- A. Normal, negatively skewed, positively skewed, skewed with outliers
- B. Skewed with outliers, positively skewed, negatively skewed, normal
- C. Normal, positively skewed, negatively skewed, normal with outliers (Correct Answer)
- D. Normal, negatively skewed, positively skewed, normal with outliers
Explanation: ### ***Normal, positively skewed, negatively skewed, normal with outliers*** - Boxplot 1 shows a relatively symmetric distribution with the median line close to the center of the box and whiskers of similar length, indicating a **normal distribution**. - Boxplot 2 has its median shifted towards the lower quartile and a longer whisker/tail on the right side, characteristic of a **positively skewed (right-skewed) distribution**. - Boxplot 3 has its median shifted towards the upper quartile and a longer whisker/tail on the left side, indicating a **negatively skewed (left-skewed) distribution**. - Boxplot 4 shows a relatively symmetric distribution, but with individual data points (represented by dots) extending beyond the whiskers, which are considered **outliers** in an otherwise **normal distribution**. ### *Normal, negatively skewed, positively skewed, skewed with outliers* - This option incorrectly identifies the skewness for plots 2 and 3. Plot 2 is positively skewed, not negatively, and plot 3 is negatively skewed, not positively. - While plot 4 does have outliers, referring to it simply as "skewed with outliers" is less precise when its central distribution appears normal. ### *Skewed with outliers, positively skewed, negatively skewed, normal* - This option incorrectly identifies plot 1 as "skewed with outliers" when it appears normal. - It also incorrectly reverses the descriptions for plot 2 (positively skewed) and plot 4 (normal with outliers). ### *Normal, negatively skewed, positively skewed, normal with outliers* - This option incorrectly identifies the skewness for plot 2, labeling it as negatively skewed instead of positively skewed. - It also incorrectly labels plot 3 as positively skewed, when it is negatively skewed.
Question 8: Which of the following is not a part of case-control studies?
- A. Strength of association
- B. Follow up (Correct Answer)
- C. Matching
- D. Selection of study subjects
Explanation: ***Follow up*** - **Follow-up** of participants over time to observe disease incidence or outcomes is a characteristic of **cohort studies**, not case-control studies. - Case-control studies are typically **retrospective**, looking back in time after disease occurrence. *Strength of association* - Measuring the **strength of association** between an exposure and an outcome using metrics like the **odds ratio** is a primary objective of case-control studies. - This helps quantify the increased risk of disease attributable to a particular exposure. *Matching* - **Matching** is a technique frequently used in case-control studies to control for **confounding variables** by selecting controls who are similar to cases in terms of age, gender, or other relevant factors. - This helps ensure that any observed association is truly due to the exposure and not other differences between the groups. *Selection of study subjects* - The **selection of study subjects** is fundamental in case-control studies, involving the identification of individuals with the disease (**cases**) and a comparable group without the disease (**controls**). - Careful selection is crucial to minimize bias and ensure the validity of the study findings.
Question 9: A new drug has been introduced into the market which was found to decrease mortality but it does not cure the disease. Which of the following is a true statement regarding prevalence and incidence?
- A. Increase in prevalence (Correct Answer)
- B. Decrease in incidence
- C. Decrease in prevalence
- D. Increase in incidence
Explanation: ***Increase in prevalence*** - A drug that decreases mortality without curing the disease means people **live longer with the condition**, thus increasing the duration of disease - **Prevalence = Incidence × Duration**: Since duration increases while incidence remains constant, prevalence increases - More existing cases accumulate over time as fewer patients die from the disease *Decrease in incidence* - **Incidence** refers to the rate at which **new cases** develop in a population - This drug affects survival of existing cases, not the development of new cases - Since the drug neither prevents nor promotes new cases, **incidence remains unchanged** (not decreased) *Decrease in prevalence* - Prevalence would decrease if the drug **cured the disease** (removing people from the diseased pool) or if **mortality increased** - The scenario describes the opposite: decreased mortality without cure, which **increases** prevalence *Increase in incidence* - This would mean more new cases are developing over time - The drug affects **survival** of existing cases, not the **rate of new diagnoses** - Incidence remains unchanged, not increased
Question 10: What is triage for?
- A. To rehabilitate following a disaster
- B. To prepare for a disaster
- C. To classify the priority of treatment (Correct Answer)
- D. To assess the impact of a disaster
Explanation: ***To classify the priority of treatment*** - **Triage** is the process of sorting patients to determine the **priority** of their treatment based on the **severity** of their condition and the likelihood of recovery, especially when resources are limited. - This system ensures that those who need immediate care most urgently receive it first, maximizing the number of lives saved. *To rehabilitate following a disaster* - **Rehabilitation** focuses on restoring health and functional abilities after an injury or illness, which occurs **post-treatment**, not as the initial classification of need. - This phase of care happens *after* triage has been completed and immediate medical needs have been addressed. *To prepare for a disaster* - **Disaster preparedness** involves planning and training *before* a disaster strikes to mitigate its effects and ensure an effective response. - Triage is a **response mechanism** utilized *during* or *immediately after* a disaster, not a preparatory measure. *To assess the impact of a disaster* - **Impact assessment** involves evaluating the damage, casualties, and overall consequences of a disaster. - While disaster impact assessment helps guide overall response, triage is specifically about **individual patient assessment** and prioritization for medical care.