All (225)Anatomy (22)Anesthesiology (4)Biochemistry (15)Community Medicine (9)Dental (1)Dermatology (4)ENT (15)Forensic Medicine (3)Internal Medicine (24)Microbiology (10)Obstetrics and Gynecology (11)Ophthalmology (23)Orthopaedics (12)Pathology (16)Pediatrics (9)Pharmacology (11)Physiology (16)Psychiatry (1)Psychiatry (3)Radiology (2)Surgery (14)
Q191
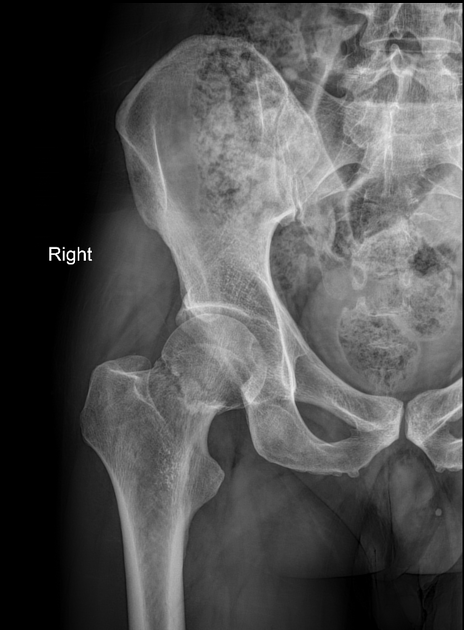
79 yrs old lady had fall, the following X-ray was taken. Which of the following is treatment?