Back
How to Study Infectious Disease for USMLE Step 2 CK: High-Yield Topics, Clinical Vignette Patterns and Exam Strategy (2026)
Master USMLE Step 2 CK infectious disease with this comprehensive guide covering high-yield organisms, antibiotic selection patterns, and clinical vignette strategies for 2026.

How to Study Infectious Disease for USMLE Step 2 CK: High-Yield Topics, Clinical Vignette Patterns and Exam Strategy (2026)
You are probably staring at another 400-page ID textbook wondering how to distill tuberculosis, meningitis, and 47 different antibiotic mechanisms into something you can actually use on exam day. Here's the truth: Step 2 CK infectious disease questions dont test your ability to memorize every organism — they test pattern recognition and clinical decision-making under pressure.
Step 2 CK devotes roughly 15-18% of questions to infectious disease, which means about 60 questions out of 318 total. Those 60 questions can make or break your score because ID intersects with every other specialty. Miss the empiric antibiotic choice for a 72-year-old with nursing home pneumonia, and you are not just losing an ID point — you are missing internal medicine, geriatrics, and clinical reasoning all at once.
The exam wants you to think like a resident on call at 2 AM: incomplete information, time pressure, and real consequences. This guide breaks down exactly how to master the high-yield organisms, recognize classic vignette patterns, and nail the antibiotic selection logic that separates 250+ scorers from the rest.
Core Study Strategy: Think Empirically First
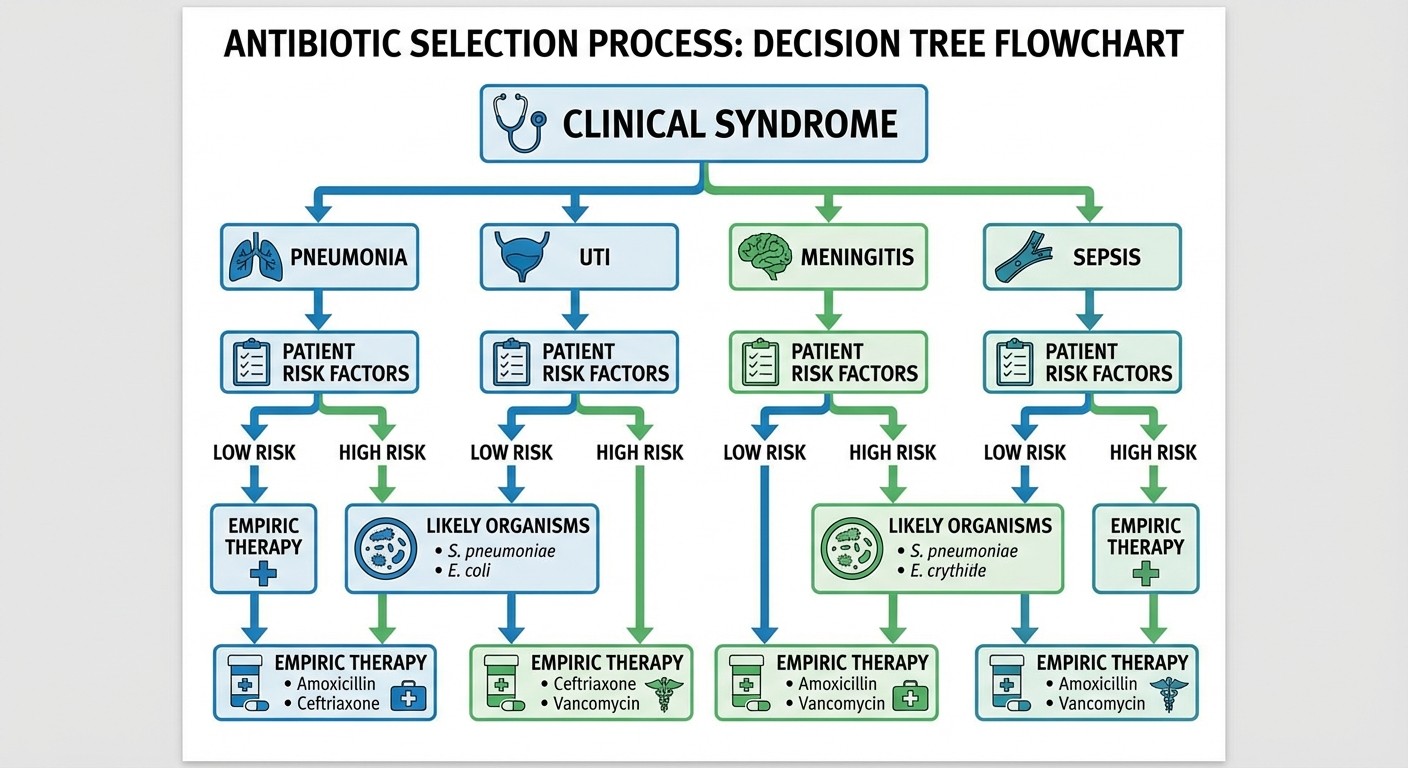
Step 2 CK infectious disease questions follow a predictable hierarchy. The vignette gives you clinical context → you identify the most likely organism → you choose empiric therapy → you adjust based on culture results. But here's where most students mess up: they try to memorize organism-antibiotic pairs instead of learning the decision tree.
The Step 2 CK infectious disease framework:
1. Clinical syndrome (pneumonia, meningitis, UTI, etc.)
2. Patient factors (age, comorbidities, healthcare exposure, immunocompromised status)
3. Most likely organisms for that syndrome + patient context
4. Empiric antibiotic coverage that hits the likely pathogens
5. Adjustment once you have culture/sensitivity data
This framework appears in every ID vignette. Master it, and you will start recognizing patterns within the first two sentences.
High-Yield Organisms and Clinical Presentations
HIV/AIDS: CD4 Counts Are Everything
HIV questions on Step 2 CK revolve around CD4 thresholds and opportunistic infection timing. You are not diagnosing HIV — you are managing complications in known HIV-positive patients.
Critical CD4 thresholds:
>500: Essentially normal immunity, typical infections
200-500: Increased bacterial infections, TB reactivation, thrush
100-200: PCP pneumonia territory (start prophylaxis at CD4 <200)
50-100: CMV retinitis, MAC, toxoplasma
<50: Everything above plus CMV colitis, cryptococcal meningitis
Classic Step 2 CK HIV vignettes:
34-year-old man with CD4 150, dry cough, bilateral infiltrates → PCP pneumonia (TMP-SMX + steroids if PaO2 <70 or A-a gradient >35)
HIV patient with CD4 80, headache, ring-enhancing lesions → Toxoplasma (sulfadiazine + pyrimethamine + leucovorin)
CD4 30, bloody diarrhea, CMV inclusion bodies → CMV colitis (ganciclovir)
The key insight: Oncourse's HIV/AIDS opportunistic infections lessons map each pathogen to specific CD4 ranges, so when you see a count, you immediately know the differential.
Pneumonia: Location Determines Pathogen
Community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP), and ventilator-associated pneumonia (VAP) have completely different organisms and treatment approaches.
CAP in healthy adults:
S. pneumoniae (still #1)
Mycoplasma pneumoniae (young adults, gradual onset, minimal sputum)
Legionella (elderly, smokers, water exposure, hyponatremia)
Chlamydophila pneumoniae (school-aged children, prolonged cough)
HAP/VAP (>48 hours in hospital):
Pseudomonas aeruginosa
Klebsiella pneumoniae
Acinetobacter
MRSA (especially if prior antibiotic exposure)
Empiric therapy decisions:
CAP outpatient: azithromycin or doxycycline
CAP inpatient: ceftriaxone + azithromycin OR respiratory fluoroquinolone
HAP/VAP: antipseudomonal beta-lactam + antipseudomonal fluoroquinolone OR aminoglycoside ± MRSA coverage
Step 2 CK loves testing the decision between empiric MRSA coverage (vancomycin or linezolid) for HAP. The triggers: ICU admission, mechanical ventilation, prior MRSA infection, or recent antibiotic exposure within 90 days.
Meningitis: Age Groups Have Different Bugs
Bacterial meningitis organisms cluster by age, and Step 2 CK questions practically hand you the age in the first sentence.
Neonates (0-3 months):
Group B Strep (S. agalactiae)
E. coli
Listeria monocytogenes
Children (3 months - 18 years):
S. pneumoniae
N. meningitidis
H. influenzae (rare post-vaccine)
Adults (18-50):
S. pneumoniae
N. meningitidis
Elderly (>50) or immunocompromised:
S. pneumoniae
N. meningitidis
Listeria monocytogenes
Empiric therapy by age:
Neonates: ampicillin + gentamicin (or ampicillin + cefotaxime)
1 month - 50 years: vancomycin + ceftriaxone
>50 years or immunocompromised: vancomycin + ampicillin + ceftriaxone
The ampicillin addition in elderly/immunocompromised patients covers Listeria, which is resistant to cephalosporins. This distinction appears frequently on Step 2 CK because students often forget the Listeria coverage gap.
STIs: Know the Stages and Treatments
Sexually transmitted infections show up in multiple specialties on Step 2 CK — internal medicine, OB/GYN, urology, and dermatology.
Gonorrhea and Chlamydia:
Often co-infected (treat both empirically)
Gonorrhea: ceftriaxone 250 mg IM × 1
Chlamydia: azithromycin 1 g PO × 1 OR doxycycline 100 mg BID × 7 days
Test of cure in pregnancy, persistent symptoms, or pharyngeal gonorrhea
Syphilis staging:
Primary: painless chancre, darkfield positive
Secondary: rash (palms/soles), condyloma lata, lymphadenopathy
Latent: asymptomatic, positive serology
Tertiary: neurosyphilis, cardiovascular, gummas
Syphilis treatment:
Primary/secondary/early latent (<1 year): benzathine penicillin G 2.4 million units IM × 1
Late latent/unknown duration: benzathine penicillin G 2.4 million units IM weekly × 3 doses
Neurosyphilis: aqueous penicillin G 18-24 million units IV daily × 10-14 days
When you practice with Oncourse's adaptive question bank, you'll notice it surfaces your specific STI knowledge gaps — like distinguishing primary syphilis from HSV or knowing when to LP for neurosyphilis — and routes you to targeted practice until mastery.
Tuberculosis: Primary vs Reactivation Patterns
TB questions test your ability to distinguish primary infection from reactivation and choose appropriate treatment regimens.
Primary TB:
Lower/middle lobe infiltrates
Hilar lymphadenopathy
More common in children, immunocompromised
Reactivation TB:
Upper lobe cavitary lesions
Adult with risk factors (HIV, diabetes, malnutrition, immunosuppression)
Latent TB testing:
IGRA (interferon-gamma release assay) preferred over PPD
Positive if ≥5 mm in HIV+ or recent close contact
Positive if ≥10 mm in high-risk groups
Positive if ≥15 mm in low-risk populations
Treatment regimens:
Active TB: RIPE (rifampin, isoniazid, pyrazinamide, ethambutol) × 2 months → rifampin + isoniazid × 4 months
Latent TB: isoniazid × 9 months OR rifampin × 4 months
Step 2 CK often tests the decision to start empiric TB treatment before culture confirmation. The trigger: HIV+ patient with upper lobe cavitary lesions and constitutional symptoms. You dont wait 6-8 weeks for culture results.
Clinical Vignette Pattern Recognition
How to Identify the Organism from Presentation Alone
Step 2 CK vignettes contain organism clues scattered throughout the clinical presentation. Learning to spot these clues early saves time and improves accuracy.
Legionella pneumonia clues:
Elderly patient
Recent travel/hotel stay
Hyponatremia
Diarrhea + pneumonia
High fever, dry cough
Pseudomonas clues:
Cystic fibrosis
Hot tub exposure
Green sputum
Healthcare exposure
Antibiotic-resistant gram-negative rods
Listeria clues:
Pregnancy
Age >65
Immunocompromised
Deli meat consumption
Ampicillin-sensitive, cephalosporin-resistant
Staphylococcus aureus clues:
IVDU (IV drug use)
Skin/soft tissue infections
Endocarditis in young patient
Post-influenza pneumonia
Group B Strep clues:
Neonatal sepsis
Postpartum endometritis
Diabetes mellitus
Elderly with cellulitis
The pattern: Step 2 CK gives you just enough clinical context to narrow down to 2-3 likely organisms, then tests whether you choose the right empiric therapy for that differential.
Empiric vs Directed Therapy Decision Logic
Step 2 CK frequently tests the timing of antibiotic decisions: when to start empirically, when to wait for cultures, and when to switch to directed therapy.
Start empiric therapy immediately:
Sepsis/septic shock
Bacterial meningitis (after blood cultures, before LP if delayed)
Neutropenic fever
Severe pneumonia with respiratory distress
Can wait for culture results:
Stable outpatient UTI
Cellulitis without systemic symptoms
Chronic infections (TB, atypical organisms)
Switch to directed therapy when:
Culture/sensitivity results available
Clinical improvement on empiric therapy (continue current)
Clinical worsening (broaden coverage or consider resistance)
The classic Step 2 CK trap: starting antibiotics before obtaining cultures in stable patients. The correct answer often involves obtaining cultures first unless the patient is unstable.
High-Yield Antibiotic Resistance Concepts
MRSA Coverage Decisions
MRSA coverage (vancomycin, linezolid, daptomycin) is expensive and has side effects, so Step 2 CK tests when to include it empirically.
Include MRSA coverage for:
Healthcare-associated infections (HAP, VAP, catheter-related)
Known MRSA colonization
Recent antibiotic exposure
ICU admission
Severe skin/soft tissue infection with systemic symptoms
Skip MRSA coverage for:
Community-acquired pneumonia in healthy adults
Simple UTI
Outpatient cellulitis without systemic symptoms
ESBL and Carbapenem Resistance
Extended-spectrum beta-lactamase (ESBL) producing organisms are increasingly common and appear on Step 2 CK in healthcare settings.
ESBL risk factors:
Recent antibiotic use (especially fluoroquinolones, 3rd generation cephalosporins)
Healthcare exposure
Nursing home residence
Indwelling devices
ESBL treatment:
Carbapenems (meropenem, imipenem, ertapenem)
Avoid cephalosporins and penicillins
The Step 2 CK pattern: elderly nursing home resident with recurrent UTI, recent cephalosporin use → suspect ESBL E. coli → start carbapenem.
System-Specific Infectious Disease Pearls
Endocarditis: Duke Criteria and Risk Stratification
Endocarditis questions test your ability to apply Duke criteria and match organisms to risk factors.
Major criteria:
Positive blood cultures (typical organisms)
Echocardiographic evidence (vegetation, abscess)
Minor criteria:
Predisposing condition (IVDU, valve disease)
Fever ≥38°C
Vascular phenomena (emboli, hemorrhage)
Immunologic phenomena (glomerulonephritis, Roth spots)
Positive blood culture not meeting major criteria
Organism-risk factor associations:
S. aureus: IVDU, acute presentation
Viridans group strep: dental procedures, gradual onset
Enterococcus: elderly, GU procedures
HACEK organisms: culture-negative, dental disease
Empiric therapy:
Native valve, acute: vancomycin + ceftriaxone
Native valve, subacute: ampicillin + gentamicin
Prosthetic valve: vancomycin + gentamicin + rifampin
UTI and Pyelonephritis: Complexity Stratification
UTI questions test your ability to distinguish simple vs complicated infections and choose appropriate therapy duration.
Simple cystitis (healthy women):
Nitrofurantoin × 5 days
TMP-SMX × 3 days
Fosfomycin × 1 dose
Complicated UTI:
Men, pregnancy, immunocompromised, structural abnormalities
Fluoroquinolone × 7 days OR TMP-SMX × 7 days (if susceptible)
Pyelonephritis:
Outpatient: fluoroquinolone × 7 days
Inpatient: ceftriaxone OR fluoroquinolone
Complicated: 14 days total
The key distinction: Step 2 CK considers ANY UTI in men as complicated and requires longer treatment duration.
Sepsis and Source Control
Sepsis questions test your understanding of empiric coverage and source control principles.
Empiric sepsis coverage:
Broad-spectrum: piperacillin-tazobactam OR cefepime OR carbapenem
Add MRSA coverage if risk factors present
Add antifungal if immunocompromised, prolonged ICU stay, or high Candida risk
Source control priorities:
Remove infected devices (catheters, prosthetics)
Drain abscesses >4 cm
Surgical debridement of necrotic tissue
Percutaneous drainage when surgery not feasible
Step 2 CK loves testing the timing of source control: antibiotics alone are insufficient for infected devices or undrained abscesses.
Travel Medicine and Geography-Specific Infections
Malaria Prophylaxis and Treatment
Travel medicine appears regularly on Step 2 CK, especially malaria prevention and recognition.
Prophylaxis by region:
Chloroquine-sensitive areas: chloroquine
Chloroquine-resistant: atovaquone-proguanil OR doxycycline OR mefloquine
Malaria treatment:
Uncomplicated: artemether-lumefantrine OR atovaquone-proguanil
Severe: artesunate (first-line) OR quinidine
Malaria clues in vignettes:
Recent travel to endemic area
Fever, chills, headache
Hemolytic anemia
Thrombocytopenia
Cyclic symptoms
Traveler's Diarrhea Patterns
Diarrheal illness questions often include travel history as the key diagnostic clue.
E. coli subtypes:
ETEC: watery diarrhea, most common traveler's diarrhea
EHEC (O157:H7): bloody diarrhea, HUS risk, avoid antibiotics
EIEC: invasive, bloody diarrhea
Geographic associations:
Campylobacter: poultry, developing countries
Salmonella: eggs, poultry, reptile exposure
Shigella: person-to-person, day-care centers
Vibrio: seafood, coastal areas
Treatment approach:
Mild: supportive care, oral rehydration
Moderate: fluoroquinolone × 3 days OR azithromycin × 3 days
Severe: hospitalization, IV fluids, culture-directed therapy
The Step 2 CK pearl: dont give antibiotics for E. coli O157:H7 (increases HUS risk). The vignette will mention bloody diarrhea + hamburger consumption + hemolytic anemia.
Fungal Infections: Immunocompromised Host Patterns
Fungal infection questions cluster around immunocompromised patients and specific geographic exposures.
Invasive Candida
Risk factors:
Prolonged ICU stay
Central venous catheter
Broad-spectrum antibiotics
TPN (total parenteral nutrition)
Recent surgery
Treatment:
Stable: fluconazole
Unstable or azole-resistant: echinocandin (caspofungin, micafungin)
Aspergillus
Risk factors:
Neutropenia
Hematologic malignancy
Lung transplant
Construction exposure
Classic presentation:
"Halo sign" on CT chest
Hemoptysis
Refractory pneumonia in neutropenic patient
Treatment:
Voriconazole (first-line)
Amphotericin B (alternative)
Geographic Fungi
Histoplasma:
Ohio/Mississippi river valleys
Bat/bird droppings
Cave exploration
Coccidioides:
Southwest US (Arizona, California)
Desert activities
"Valley fever"
Blastomyces:
Great Lakes region
Outdoor activities
Skin lesions + pulmonary
When practicing infectious disease flashcards, you'll notice Oncourse uses spaced repetition to reinforce these geography-organism associations, which are pure memorization but high-yield for Step 2 CK.
Study Schedule and Resource Integration
Month 1: Foundation Building
Week 1-2: Core concepts
HIV opportunistic infections by CD4 count
Pneumonia pathogen-location associations
Basic antibiotic mechanisms and spectra
Week 3-4: Pattern recognition
Meningitis by age group
STI presentations and staging
Endocarditis organism-risk factor pairs
Use Oncourse's pediatric infectious disease lessons alongside internal medicine content to see how age affects pathogen distribution across specialties.
Month 2: Clinical Integration
Week 1-2: Antibiotic selection logic
Empiric vs directed therapy timing
MRSA coverage decisions
Resistance pattern recognition
Week 3-4: Specialty crossover
ID in pregnancy (GBS, listeria, syphilis)
ID in surgery (prophylaxis, post-op infections)
ID in ICU (HAP, VAP, fungal)
Oncourse's AI explanations map each answer choice to real clinical scenarios, so you learn why empiric vancomycin + piperacillin-tazobactam covers both MRSA and Pseudomonas in HAP, not just that it does.
Final Month: Synthesis and Speed
Week 1-2: Vignette drills
Timed practice focusing on pattern recognition
Classic Step 2 CK traps and distractors
Source control and non-antibiotic management
Week 3-4: Weak area reinforcement
Use Oncourse's performance analytics to identify gaps
Focus on missed organism-syndrome associations
Review travel medicine and geographic fungi
The adaptive question bank surfaces your specific weaknesses — maybe you keep confusing Legionella vs Mycoplasma pneumonia patterns — and auto-routes you to targeted practice until you've hit mastery.
High-Yield Organisms Summary Table
Organism | Classic Presentation | First-Line Treatment | Key Clue |
|---|---|---|---|
S. pneumoniae | CAP, meningitis | Ceftriaxone | Gram+ diplococci, rusty sputum |
MRSA | Healthcare infections | Vancomycin | Recent antibiotics, ICU exposure |
Pseudomonas | CF, hot tubs, HAP | Antipseudomonal beta-lactam | Green sputum, healthcare setting |
Legionella | Hotel stay, elderly | Azithromycin | Hyponatremia, atypical pneumonia |
Listeria | Pregnancy, elderly | Ampicillin | Deli meat, immunocompromised |
N. meningitidis | Young adults, dorms | Ceftriaxone | Petechial rash, close contacts |
C. difficile | Recent antibiotics | Vancomycin PO | Pseudomembranes, recent clindamycin |
PCP | HIV, CD4 <200 | TMP-SMX | Dry cough, bilateral infiltrates |
Cryptococcus | HIV, CD4 <100 | Amphotericin B + flucytosine | Headache, India ink positive |
Candida | ICU, catheters | Fluconazole | Pseudohyphae, risk factors |
Frequently Asked Questions
How much detail should I know about antibiotic mechanisms?
Step 2 CK focuses on antibiotic selection, not mechanisms. Know spectrum coverage (gram-positive vs gram-negative, aerobic vs anaerobic) and major resistance patterns (MRSA, ESBL, VRE). Skip the detailed pharmacokinetics unless it affects clinical decision-making (like CNS penetration for meningitis).
What's the best way to memorize CD4 count thresholds for HIV?
Use the "countdown" method: Start at 500 (normal immunity) and count down by major intervals. 200 = PCP territory, 100 = CMV/MAC territory, 50 = everything territory. Practice HIV opportunistic infection questions until the associations become automatic.
Should I memorize antibiotic dosing and duration?
Focus on treatment duration over exact dosing. Step 2 CK cares more about whether you choose 3 days vs 7 days vs 14 days for UTI than the exact milligrams. Dosing details appear only when clinically relevant (like high-dose penicillin for neurosyphilis).
How do I distinguish between similar-presenting infections?
Look for discriminating features: Legionella has hyponatremia + atypical pneumonia, Mycoplasma affects young adults with gradual onset, Chlamydophila causes prolonged cough in school-age children. The vignette always provides enough context to differentiate — trust the clinical clues.
What should I do if I cant identify the organism from the vignette?
Fall back to empiric therapy for the clinical syndrome. Step 2 CK sometimes gives vague presentations specifically to test your empiric decision-making. Know the empiric coverage for pneumonia, meningitis, sepsis, and UTI by patient age and risk factors.
How important are culture interpretation and lab values?
Very important. Step 2 CK expects you to interpret CSF findings (bacterial vs viral meningitis), blood culture results (significance of gram-positive cocci vs gram-negative rods), and basic lab patterns (elevated WBC with left shift suggests bacterial infection). Practice recognizing normal vs abnormal lab patterns for each infection type.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.