
Opportunistic infections in HIV/AIDS — MCQs

A 26-year-old man comes to the physician for a follow-up examination. He was diagnosed with HIV infection 2 weeks ago. His CD4+ T-lymphocyte count is 162/mm3 (N ≥ 500). An interferon-gamma release assay is negative. Prophylactic treatment against which of the following pathogens is most appropriate at this time?
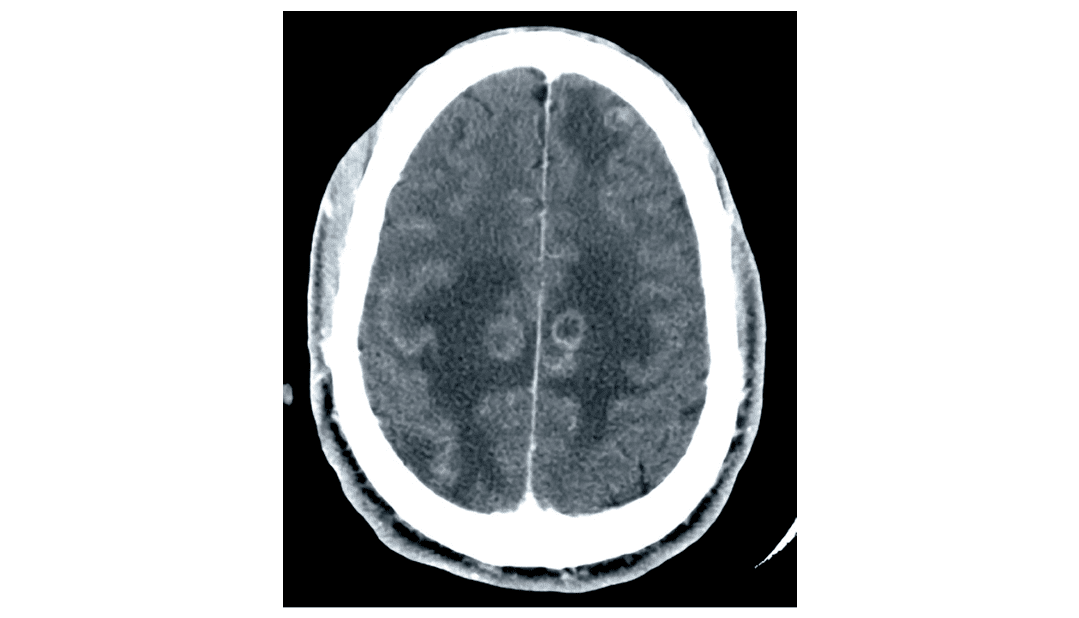
A 35-year-old man is brought to the emergency department after experiencing a seizure. According to his girlfriend, he has had fatigue for the last 3 days and became confused this morning, after which he started having uncontrollable convulsions throughout his entire body. He was unconscious throughout the episode, which lasted about 4 minutes. He has not visited a physician for over 10 years. He has smoked one pack of cigarettes daily for 12 years. His girlfriend admits they occasionally use heroin together with their friends. His temperature is 38.8°C (101.8°F), pulse is 93/min, respirations are 20/min, and blood pressure is 110/70 mm Hg. The lungs are clear to auscultation and examination shows normal heart sounds and no carotid or femoral bruits. He appears emaciated and somnolent. There are multiple track marks on both his arms. He is unable to cooperate for a neurological exam. Laboratory studies show a leukocyte count of 3,000/mm3, a hematocrit of 34%, a platelet count of 354,000/mm3, and an erythrocyte sedimentation rate of 27 mm/h. His CD4+ T-lymphocyte count is 84/mm3 (normal ≥ 500). A CT scan of the head is shown. Which of the following is the most appropriate next step considering this patient's CT scan findings?
A 40-year-old man with AIDS comes to the physician because of a 3-week history of intermittent fever, abdominal pain, and diarrhea. He has also had a nonproductive cough and a 3.6-kg (8-lb) weight loss in this period. He was treated for pneumocystis pneumonia 2 years ago. He has had skin lesions on his chest for 6 months. Five weeks ago, he went on a week-long hiking trip in Oregon. Current medications include efavirenz, tenofovir, and emtricitabine. He says he has had trouble adhering to his medication. His temperature is 38.3°C (100.9°F), pulse is 96/min, and blood pressure is 110/70 mm Hg. Examination shows oral thrush on his palate and a white, non-scrapable plaque on the left side of the tongue. There is axillary and inguinal lymphadenopathy. There are multiple violaceous plaques on the chest. Crackles are heard on auscultation of the chest. Abdominal examination shows mild, diffuse tenderness throughout the lower quadrants. The liver is palpated 2 to 3 cm below the right costal margin, and the spleen is palpated 1 to 2 cm below the left costal margin. Laboratory studies show: Hemoglobin 12.2 g/dL Leukocyte count 4,800/mm3 CD4+ T-lymphocytes 44/mm3 (Normal ≥ 500 mm3) Platelet count 258,000/mm3 Serum Na+ 137 mEq/L Cl- 102 mEq/L K+ 4.9 mEq/L Alkaline phosphatase 202 U/L One set of blood culture grows acid-fast organisms. A PPD skin test shows 4 mm of induration. Which of the following is the most appropriate pharmacotherapy for this patient's condition?
A 35-year-old man comes to the emergency department with fever, chills, dyspnea, and a productive cough. His symptoms began suddenly 2 days ago. He was diagnosed with HIV 4 years ago and has been on triple antiretroviral therapy since then. He smokes one pack of cigarettes daily. He is 181 cm (5 ft 11 in) tall and weighs 70 kg (154 lb); BMI is 21.4 kg/m2. He lives in Illinois and works as a carpenter. His temperature is 38.8°C (101.8°F), pulse is 110/min, respirations are 24/min, and blood pressure is 105/74 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 92%. Examinations reveals crackles over the right lower lung base. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.5 g/dL Leukocyte count 12,800/mm3 Segmented neutrophils 80% Eosinophils 1% Lymphocytes 17% Monocytes 2% CD4+ T-lymphocytes 520/mm3(N ≥ 500) Platelet count 258,000/mm3 Serum Na+ 137 mEq/L Cl- 102 mEq/L K+ 5.0 mEq/L HCO3- 22 mEq/L Glucose 92 mg/dL An x-ray of the chest shows a right lower-lobe infiltrate of the lung. Which of the following is the most likely causal organism?
A 33-year-old man with HIV comes to the physician because of a nonproductive cough and shortness of breath for 3 weeks. He feels tired after walking up a flight of stairs and after long conversations on the phone. He appears chronically ill. His temperature is 38.5°C (101.3°F), and pulse is 110/min. Pulse oximetry on room air shows an oxygen saturation of 95%. Upon walking, his oxygen saturation decreases to 85%. Cardiopulmonary examination is normal. Laboratory studies show a CD4+ T-lymphocyte count of 176/mm3 (N > 500). Results of urine Legionella antigen testing are negative. A CT scan of the chest shows diffuse, bilateral ground-glass opacities. Microscopic examination of fluid obtained from bronchoalveolar lavage will most likely show which of the following findings?
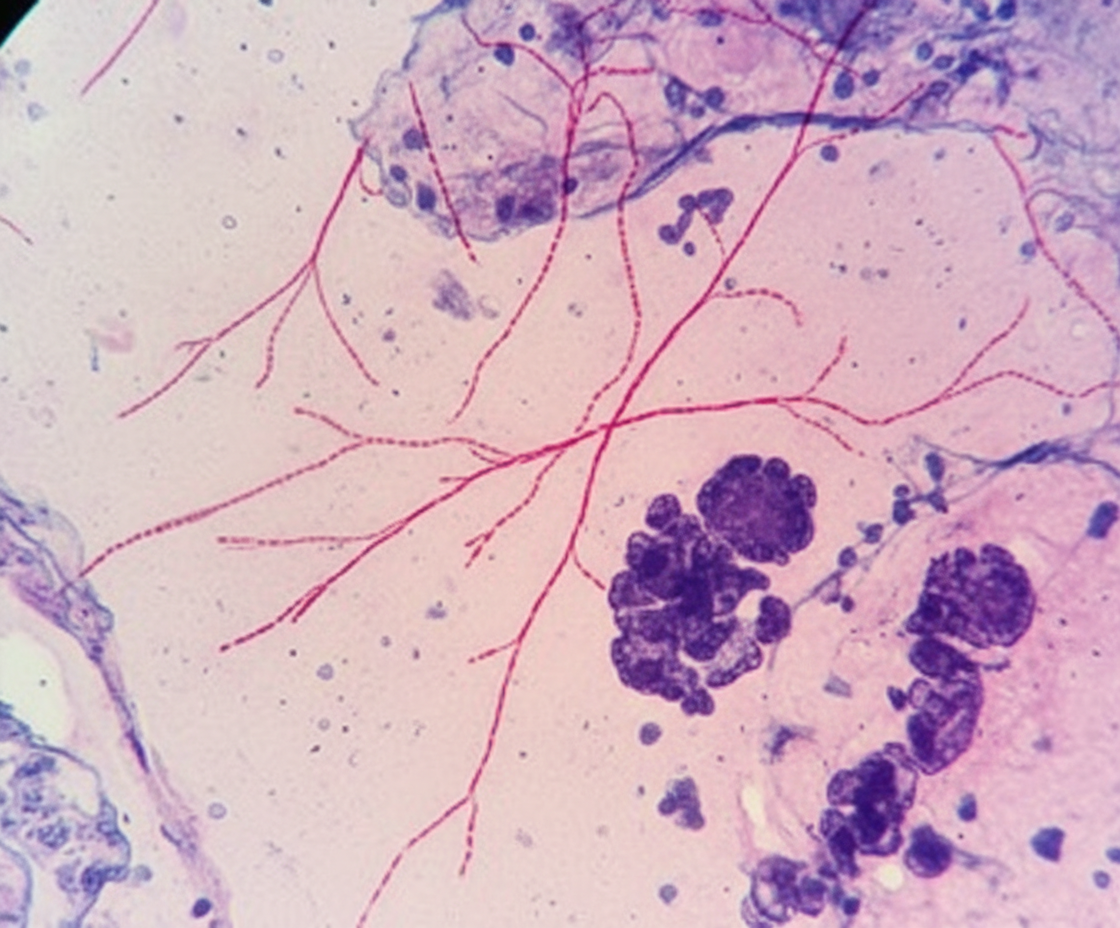
A 68-year-old man comes to the physician because of a 1-month history of fatigue, low-grade fevers, and cough productive of blood-tinged sputum. He has type 2 diabetes mellitus and chronic kidney disease and underwent kidney transplantation 8 months ago. His temperature is 38.9°C (102.1°F) and pulse is 98/min. Examination shows rhonchi in the right lower lung field. An x-ray of the chest shows a right-sided lobar consolidation. A photomicrograph of specialized acid-fast stained tissue from a blood culture is shown. Which of the following is the strongest predisposing factor for this patient's condition?
A 34-year-old woman presents with confusion, drowsiness, and headache. The patient’s husband says her symptoms began 2 days ago and have progressively worsened with an acute deterioration of her mental status 2 hours ago. The patient describes the headaches as severe, localized to the frontal and periorbital regions, and worse in the morning. Review of symptoms is significant for a mild, low-grade fever, fatigue, and nausea for the past week. Past medical history is significant for HIV infection for which she is not currently receiving therapy. Her CD4+ T cell count last month was 250/mm3. The blood pressure is 140/85 mm Hg, the pulse rate is 90/min, and the temperature is 37.7°C (100.0°F). On physical examination, the patient is conscious but drowsy. Papilledema is present. No pain is elicited with extension of the leg at the knee joint. The remainder of the physical examination is negative. Laboratory findings, including panculture, are ordered. A noncontrast CT scan of the head is negative and is followed by a lumbar puncture. CSF analysis is significant for: Opening pressure 250 mm H2O (70-180 mm H2O) Glucose 30 mg/dL (40-70 mg/dL) Protein 100 mg/dL (<40 mg/dL) Cell count 20/mm3 (0-5/mm3) Which of the following additional findings would most likely be found in this patient?
A 41-year-old HIV-positive male presents to the ER with a 4-day history of headaches and nuchal rigidity. A lumbar puncture shows an increase in CSF protein and a decrease in CSF glucose. When stained with India ink, light microscopy of the patient’s CSF reveals encapsulated yeast with narrow-based buds. Assuming a single pathogenic organism is responsible for this patient’s symptoms, which of the following diagnostic test results would also be expected in this patient?
A 32-year-old HIV positive male presents to the office complaining of difficulty swallowing and bad breath for the past couple of months. Upon further questioning, he says, "it feels like there’s something in my throat". He says that the difficulty is sometimes severe enough that he has to skip meals. He added that it mainly occurs with solid foods. He is concerned about his bad breath since he has regular meetings with his clients. Although he is on antiretroviral medications, he admits that he is noncompliant. On examination, the patient is cachectic with pale conjunctiva. On lab evaluation, the patient’s CD4+ count is 70/mm3. What is the most likely cause of his symptoms?
A 33-year-old HIV-positive male is seen in clinic for follow-up care. When asked if he has been adhering to his HIV medications, the patient exclaims that he has been depressed, thus causing him to not take his medication for six months. His CD4+ count is now 33 cells/mm3. What medication(s) should he take in addition to his anti-retroviral therapy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app