Back
Thoracic Dermatomes and Myotomes: Complete Anatomy Guide for USMLE Step 1 and Step 2 CK (2026)
Master T1-T12 thoracic dermatomes and myotomes with clinical landmarks (T4=nipple, T10=umbilicus), spinal cord injury assessment, and high-yield USMLE patterns for Step 1 and Step 2 CK success.
Thoracic Dermatomes and Myotomes: Complete Anatomy Guide for USMLE Step 1 and Step 2 CK (2026)
You are probably staring at a dermatome map right now wondering how youll memorize 12 thoracic levels without mixing them up. The USMLE loves testing dermatome patterns — they show up in Step 1 anatomy questions and Step 2 CK clinical scenarios about spinal cord injuries, herpes zoster, and nerve blocks.
Here's the reality: thoracic dermatomes follow predictable patterns once you know the clinical landmarks. T4 hits the nipple line. T10 circles the umbilicus. T12 runs along the inguinal ligament. Master these anchor points and the rest falls into place.
This guide breaks down T1-T12 dermatomes and myotomes with the clinical correlations that matter for USMLE success. No theoretical fluff — just the high-yield patterns examiners test and how to apply them when assessing spinal cord injury levels or mapping herpes zoster distributions.
Understanding Thoracic Dermatomes: The Fundamentals
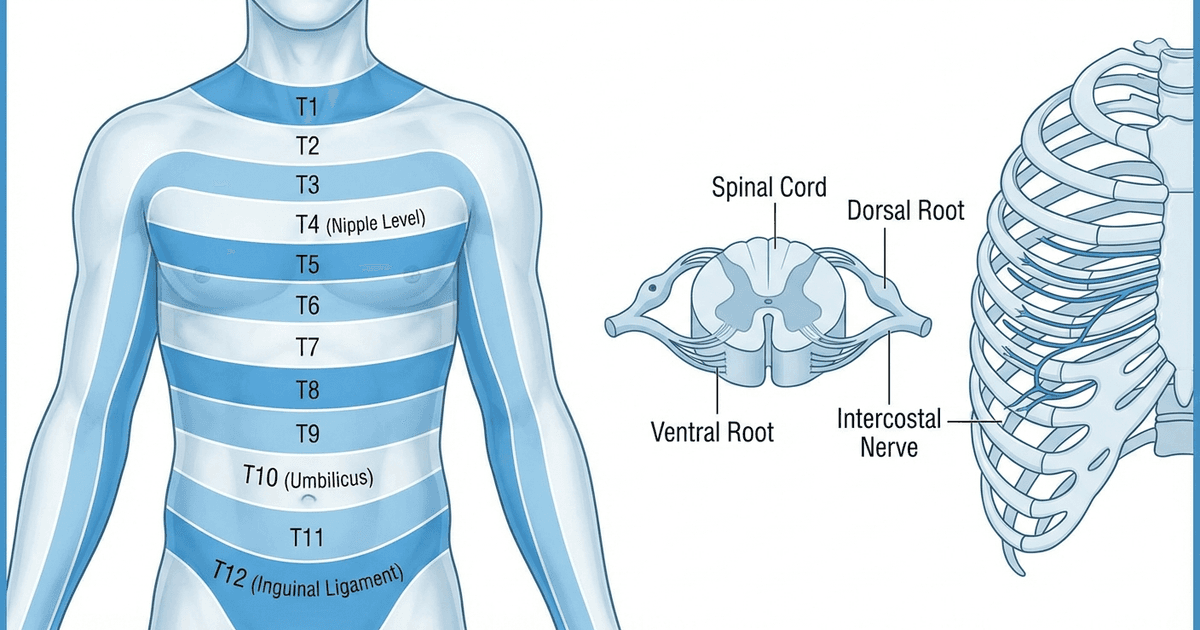
Thoracic dermatomes represent the sensory distribution of the 12 thoracic spinal nerves (T1-T12). Unlike cervical and lumbar dermatomes that form complex patterns in the extremities, thoracic dermatomes create horizontal bands around the trunk — making them easier to memorize and clinically assess.
Each thoracic nerve emerges from the spinal cord and divides into:
Dorsal ramus: Innervates the skin over the spinous processes
Ventral ramus: Forms the intercostal nerve, providing sensory innervation to the lateral and anterior chest wall
The key insight for USMLE questions: thoracic dermatomes overlap by approximately 50%. This means sensory loss from a single nerve injury often goes unnoticed clinically — but complete dermatome loss indicates spinal cord pathology at that level.
Critical Clinical Landmarks (High-Yield for USMLE)
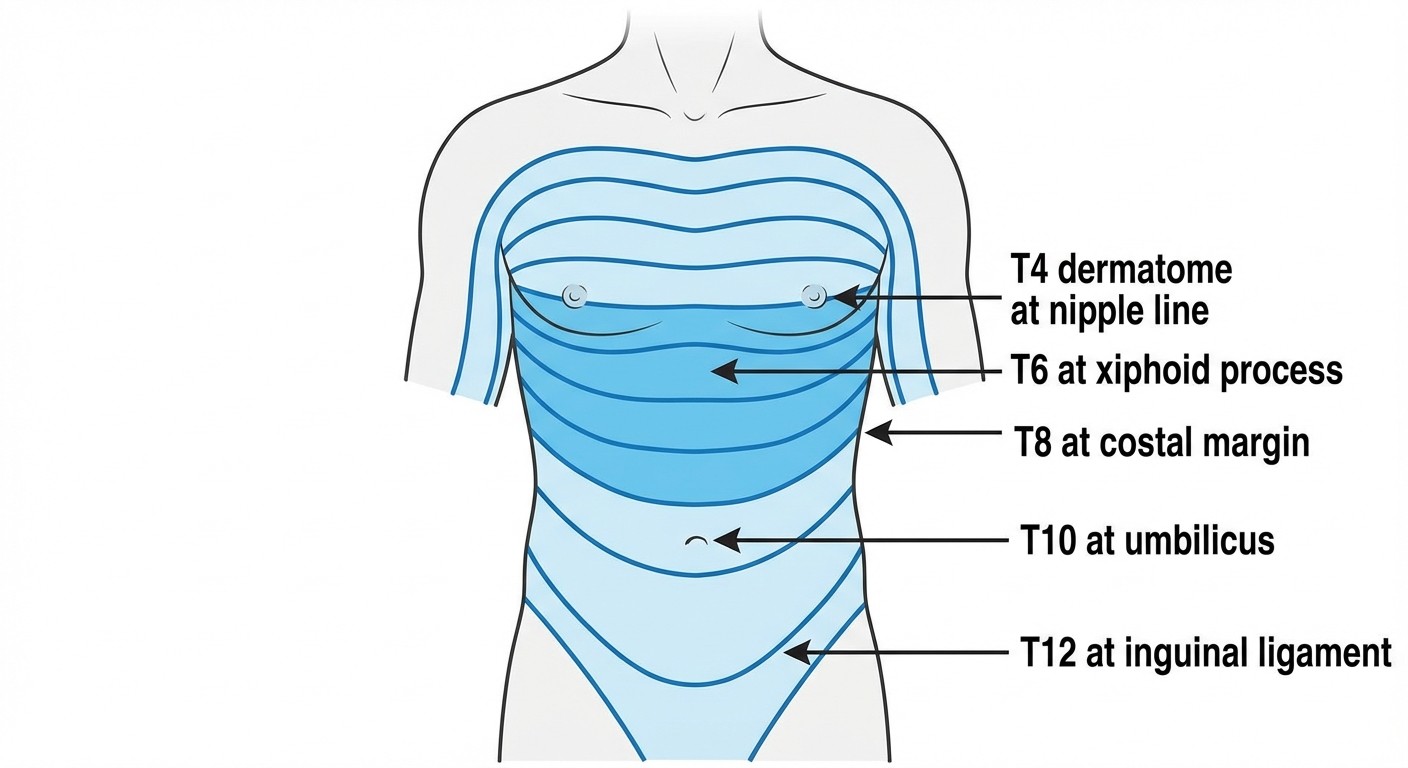
Memorize these anchor points — they appear repeatedly in USMLE questions:
Dermatome | Clinical Landmark | Clinical Significance |
|---|---|---|
T4 | Nipple line | Cardiac pain referral, breast surgery |
T6 | Xiphoid process | Gallbladder pain referral |
T8 | Costal margin | Liver edge palpation |
T10 | Umbilicus | Appendicitis pain referral |
T12 | Inguinal ligament | Transition to lumbar region |
Memory trick: "4 Nipples, 6 Xiphoid, 8 Costal, 10 Umbilicus, 12 Inguinal" — practice this sequence until automatic.
Complete T1-T12 Dermatome Mapping
Upper Thoracic (T1-T4)
T1 Dermatome:
Distribution: Medial arm and forearm, medial hand (little finger side)
Overlap: Connects with C8 and T2
Clinical note: Often involved in Horner's syndrome (sympathetic chain disruption)
T2 Dermatome:
Distribution: Medial upper arm, axilla, upper chest
Clinical correlation: Cardiac pain often refers to this region
Testing: Light touch along the axillary fold
T3 Dermatome:
Distribution: Upper chest, just above nipple line
Clinical note: Breast surgery complications may affect this level
Anatomical landmark: Third intercostal space
T4 Dermatome (High-yield):
Distribution: Nipple line, fourth intercostal space
USMLE favorite: Most tested thoracic landmark
Clinical applications: Cardiac catheterization site, breast examination reference
Middle Thoracic (T5-T8)
T5 Dermatome:
Distribution: Between nipple and xiphoid process
Clinical correlation: Sometimes involved in atypical cardiac pain
Anatomical reference: Fifth intercostal space
T6 Dermatome:
Distribution: Xiphoid process level
Clinical significance: Gallbladder pain referral pattern
USMLE context: Cholecystitis presentations
T7 Dermatome:
Distribution: Between xiphoid and costal margin
Clinical note: Pancreatic pain may refer here
Testing: Midway between T6 and T8 landmarks
T8 Dermatome:
Distribution: Costal margin, lower chest
Clinical correlation: Liver examination reference point
Anatomical landmark: Eighth intercostal space
Lower Thoracic (T9-T12)
T9 Dermatome:
Distribution: Between costal margin and umbilicus
Clinical significance: Upper abdominal assessment
Testing: Midway between T8 and T10 landmarks
T10 Dermatome (High-yield):
Distribution: Umbilicus level
USMLE favorite: Second most tested thoracic landmark
Clinical applications: Appendicitis pain assessment, abdominal examination
T11 Dermatome:
Distribution: Between umbilicus and inguinal ligament
Clinical correlation: Lower abdominal pain assessment
Anatomical reference: Eleventh intercostal space
T12 Dermatome:
Distribution: Inguinal ligament, suprapubic region
Clinical significance: Transition to lumbar dermatomes
USMLE context: Spinal cord injury level assessment
Study these patterns with thoracic dermatomes and myotomes lessons for detailed anatomical correlations.
Thoracic Myotomes: Motor Function Patterns
Thoracic myotomes differ significantly from cervical and lumbar patterns. T1-T12 primarily innervate:
T1 Myotome (Overlap with C8)
Muscles: Small muscles of the hand, interossei, lumbricals
Testing: Finger abduction/adduction, grip strength
Clinical significance: Klumpke's palsy, thoracic outlet syndrome
T2-T12 Myotomes
Primary function: Intercostal muscles, accessory respiratory muscles
Motor testing: Limited — mainly assessed through respiratory function
Clinical applications:
- Paradoxical breathing patterns in high spinal cord injuries
- Intercostal muscle paralysis assessment
- Respiratory compromise prediction
Key insight: Unlike extremity myotomes, thoracic motor testing focuses on respiratory muscle function rather than specific muscle group strength.
Practice motor testing techniques with motor testing of myotomes interactive modules.
Clinical Applications: High-Yield USMLE Scenarios
Spinal Cord Injury Level Assessment
Scenario: Complete spinal cord transection produces predictable sensory and motor loss patterns. Assessment strategy: 1. Test bilateral sensation at T4 (nipple), T10 (umbilicus), T12 (inguinal) 2. Check motor function below the level of injury 3. Assess autonomic function (temperature regulation, bladder control) USMLE pearl: Injury at T6 level preserves upper limb function but affects intercostal muscles — compromising cough reflex and respiratory reserve.
Herpes Zoster Distribution Patterns
Herpes zoster follows dermatome patterns exactly — making thoracic dermatomes clinically relevant for diagnosis.
Common presentations:
T5-T9: Most frequent thoracic zoster locations
Unilateral distribution: Never crosses midline
Pain precedes rash by 2-3 days typically
Diagnosis criteria:
Vesicular rash in dermatomal pattern
Severe burning pain
Usually affects one dermatome (occasionally two adjacent)
USMLE context: Question stems often describe unilateral chest pain with vesicular rash — expect dermatome mapping questions.
Intercostal Nerve Blocks
Understanding thoracic dermatome anatomy guides intercostal nerve block procedures and predicts anesthesia patterns.
Technical considerations:
Block location: Posterior axillary line, inferior border of rib
Anesthesia pattern: One dermatome plus overlap zones
Multiple levels: Required for larger surgical areas
Clinical applications:
Post-thoracotomy pain management
Rib fracture analgesia
Breast surgery procedures
USMLE relevance: Questions about regional anesthesia complications and distribution patterns.
Diabetic Neuropathy Patterns
Diabetic thoracic radiculopathy presents as unilateral chest or abdominal pain following dermatome distributions.
Characteristic features:
Acute onset severe pain
Dermatomal distribution (often T6-T12)
Motor weakness in affected myotomes
Gradual resolution over months
Diagnostic challenge: Often mistaken for cardiac, pulmonary, or abdominal pathology. USMLE pearl: Consider diabetic radiculopathy when patients with diabetes present with unexplained dermatomal pain patterns.
Reinforce these clinical correlations using spinal cord injury levels and their effects practice questions.
USMLE High-Yield Testing Patterns
Step 1 Anatomy Focus Areas
Direct anatomy questions:
Dermatome-landmark correlations (especially T4, T10)
Spinal nerve anatomy and branching patterns
Intercostal nerve courses and distributions
Clinical correlation questions:
Spinal cord injury level prediction from sensory loss
Herpes zoster dermatomal patterns
Pain referral patterns to thoracic dermatomes
Step 2 CK Clinical Applications
Patient presentations:
Trauma victims with spinal cord injuries
Elderly patients with herpes zoster
Diabetic patients with radiculopathy
Post-surgical pain management scenarios
Assessment scenarios:
Neurological examination techniques
Sensory level documentation
Motor function testing in spinal injuries
Treatment considerations:
Regional anesthesia planning
Pain management strategies
Rehabilitation planning for spinal cord injuries
Test your understanding with dermatomes and myotomes practice questions covering both Step 1 and Step 2 CK content.
Memory Techniques and Study Strategies
The "4-6-8-10-12" Rule
Create a visual map linking numbers to landmarks:
4: Four fingers = nipple level
6: Six pack abs start = xiphoid
8: Ate too much = costal margin (stomach)
10: Perfect 10 belly button = umbilicus
12: Twelve o'clock position = inguinal ligament
Anatomical Storytelling
"Starting at the nipples (T4), move down to the stomach (T6-T8), then the belly button (T10), and finally the bikini line (T12)."
This narrative creates a logical progression that's harder to forget under exam pressure.
Clinical Correlation Method
Link each landmark to its most important clinical correlation:
T4: Heart problems → nipple line
T6: Gallbladder pain → xiphoid
T8: Liver exam → costal margin
T10: Appendix pain → umbilicus
T12: Hip problems → inguinal ligament
Active Recall Testing
Practice without looking at references:
1. Draw a human torso outline
2. Mark T4, T6, T8, T10, T12 landmarks
3. Add clinical correlations for each level
4. Check accuracy against anatomical references
Use dermatomes and myotomes flashcards for spaced repetition practice.
How Oncourse AI Reinforces Dermatome Learning
Oncourse's adaptive anatomy module uses several techniques to make thoracic dermatome patterns stick:
Pattern Recognition Training: The AI presents dermatome questions in varying formats — from basic landmark identification to complex clinical scenarios. This builds pattern recognition across different question types you'll see on USMLE. Adaptive Spacing: Questions about commonly confused levels (like T6 vs T8) appear more frequently until you demonstrate mastery. The algorithm identifies your weak spots and targets them specifically. Clinical Integration: Instead of isolated anatomy facts, Oncourse links dermatome patterns to clinical presentations. You'll practice identifying spinal cord injury levels from symptom patterns, mapping herpes zoster distributions, and planning intercostal nerve blocks. Visual Learning: Interactive anatomy diagrams let you click and test dermatome boundaries. This active engagement builds stronger memory traces than passive reading. Immediate Feedback: When you miss a dermatome question, Oncourse's AI explains not just the correct answer, but why the other options are wrong and how to avoid similar mistakes. Cross-System Connections: The platform connects dermatome anatomy to related topics — pain physiology, spinal cord pathways, and clinical neurology — building comprehensive understanding rather than isolated facts.
Access these features through Oncourse's anatomy learning modules designed specifically for USMLE success.
Advanced Clinical Correlations
Autonomic Innervation Patterns
Thoracic spinal cord injuries affect sympathetic nervous system function predictably:
T1-T5 injuries:
Horner's syndrome risk (T1)
Cardiac sympathetic denervation
Impaired temperature regulation
T6-T12 injuries:
Preserved upper body thermoregulation
Compromised lower body autonomic function
Potential for autonomic dysreflexia
Respiratory Compromise Prediction
Understanding thoracic myotome patterns helps predict respiratory function after spinal cord injury:
C5-C7 complete injuries:
Diaphragm preserved (phrenic nerve C3-C5)
All intercostal muscles lost
Severely compromised cough and respiratory reserve
T1-T6 complete injuries:
Some upper intercostal function preserved
Better respiratory reserve than higher injuries
Still significant cough impairment
T7-T12 complete injuries:
Most intercostal muscles preserved
Near-normal respiratory function
Minimal pulmonary complications
Pain Referral Patterns
Visceral organs refer pain to predictable thoracic dermatomes:
Organ | Primary Referral | Mechanism |
|---|---|---|
Heart | T1-T5 (left > right) | Sympathetic fibers |
Lungs | T2-T6 | Sympathetic pathways |
Gallbladder | T6-T9 (right) | Visceral afferents |
Pancreas | T6-T10 | Celiac plexus |
Kidneys | T10-L1 | Sympathetic chain |
USMLE applications: Questions often test your ability to predict pain location based on organ pathology.
Frequently Asked Questions
Which thoracic dermatome landmarks are most important for USMLE?
T4 (nipple line) and T10 (umbilicus) appear most frequently in USMLE questions. T6 (xiphoid) and T12 (inguinal ligament) are also high-yield. Focus your memorization efforts on these four levels first.
How do thoracic dermatome patterns differ from cervical and lumbar?
Thoracic dermatomes form horizontal bands around the trunk, making them more predictable than the complex patterns in extremities. They show significant overlap (about 50%), so single nerve injuries rarely cause complete sensory loss.
What's the best way to test thoracic dermatome sensation clinically?
Use light touch or pin-prick testing along the midclavicular line. Test bilateral sensation at T4, T6, T8, T10, and T12 landmarks. Always compare left and right sides for asymmetry.
How reliable are thoracic dermatome maps for clinical use?
Individual variation exists, but the major landmarks (T4, T10) are consistent across >90% of people. Use dermatome maps as guides rather than absolute boundaries, especially in clinical practice.
What thoracic dermatome concepts appear most on Step 2 CK?
Step 2 CK emphasizes clinical applications: spinal cord injury assessment, herpes zoster diagnosis, intercostal nerve blocks, and pain referral patterns. Focus on practical assessment techniques rather than pure anatomy.
How do thoracic myotomes differ from other spinal levels?
Thoracic myotomes primarily control intercostal and accessory respiratory muscles rather than limb movements. Motor testing focuses on respiratory function assessment rather than specific muscle strength testing.
Master thoracic dermatome patterns systematically and they become powerful tools for USMLE success. The key is linking anatomical landmarks to clinical applications — exactly what high-scoring students do.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 1 and Step 2 CK. Download free on Android and iOS.