How to Study Orthopedics for NEET PG 2026: High-Yield Topics, Fracture Classifications and Exam Checklist
Master NEET PG orthopedics with high-yield topics, essential fracture classifications (Garden, Salter-Harris, Gustilo-Anderson), image-based questions, and a complete 30-day study plan for 2026.
How to Study Orthopedics for NEET PG 2026: High-Yield Topics, Fracture Classifications and Exam Checklist
You probably opened this thinking orthopedics is just memorizing fracture classifications. Wrong. NEET PG orthopedics in 2026 carries 12-15 questions worth 52-65 marks. That's more than entire subjects like microbiology. Yet most students treat it as an afterthought until month 3 when panic hits.
Here's what actually happens: you cram Salter-Harris, Garden, and AO classifications without understanding the clinical reasoning. Come exam day, they dont ask "What is Garden 2?" They show an X-ray of a 67-year-old with hip pain and ask about surgical approach. The classification was just foundation knowledge.
The students who score 13/15 in orthopedics dont memorize more — they pattern-match faster. They recognize injury mechanisms, predict complications, and think in treatment algorithms. This guide shows you exactly how to build that clinical intuition in the time you actually have.
Understanding NEET PG Orthopedics: What You're Really Up Against
NEET PG orthopedics follows a predictable pattern. NBE loves testing:
Trauma (40% of questions): Fracture classifications, management protocols, complications
Pediatric orthopedics (25%): Developmental dysplasia, growth plate injuries, congenital conditions
Spine (15%): Disc diseases, spinal deformities, infections
Sports medicine (10%): Ligament injuries, arthroscopy
Bone tumors (10%): Primary and metastatic, staging systems
The catch? They rarely ask straightforward factual recalls. Instead, expect case-based scenarios where you apply classifications to make treatment decisions.
High-Yield Topics That Actually Show Up
Trauma and Fractures (Must-Know Areas)
Hip Fractures and Classifications
Garden classification isnt just 1-4 numbering. Garden 1-2 are stable (can try screws), Garden 3-4 are unstable (need replacement in elderly). The real question they ask: "72-year-old fell, X-ray shows displaced femoral neck fracture, what surgery?" Answer needs Garden classification knowledge but tests surgical decision-making.
Master these trauma patterns:
Colles vs Smith fractures: Mechanism matters (FOOSH vs fall on flexed wrist)
Supracondylar fractures: Gartland classification determines treatment
Ankle fractures: Lauge-Hansen classification based on injury mechanism
Pelvic fractures: Young-Burgess classification drives management
Study fracture patterns with orthopedics trauma lessons that show X-rays alongside classifications, not just text descriptions.
Open Fractures
Gustilo-Anderson classification is high-yield, but they test it through management scenarios. Grade 1 gets immediate irrigation and debridement. Grade 3C needs vascular repair within 6 hours. Know the timeline protocols, not just the grades.
Pediatric Orthopedics (Frequent Topic)
Developmental Dysplasia of Hip (DDH)
Appears in 2-3 questions yearly. Know Barlow and Ortolani tests, but more importantly understand treatment by age:
0-6 months: Pavlik harness
6-18 months: Closed reduction + spica cast
>18 months: Open reduction
Growth Plate Injuries
Salter-Harris classification is basic. The real test is prognosis and treatment:
Type 1-2: Usually good outcome
Type 3-4: Involve joint, may need surgery
Type 5: Crush injury, worst prognosis
Practice with pediatric orthopedics flashcards that connect classification to long-term outcomes.
Spine Pathology
Disc Diseases
Distinguish herniation levels by dermatomes and reflexes. L4-L5 affects L5 nerve (dorsiflexion weakness). L5-S1 affects S1 nerve (plantar flexion weakness). They test this through clinical vignettes, not anatomy questions.
Scoliosis
Cobb angle determines treatment:
<25°: Observation
25-45°: Bracing (if skeletally immature)
>45°: Surgery
Bone Tumors
Primary Bone Tumors
Location patterns are testable:
Osteosarcoma: Around knee (distal femur, proximal tibia)
Ewing sarcoma: Diaphysis of long bones
Giant cell tumor: Epiphysis after closure
Metastatic Bone Disease
Most common primaries: Breast, lung, prostate, kidney, thyroid. Remember "BLT with a Pickle and Ketchup."
Essential Fracture Classifications You Must Master
The Big 5 Classifications (Appear Every Year)
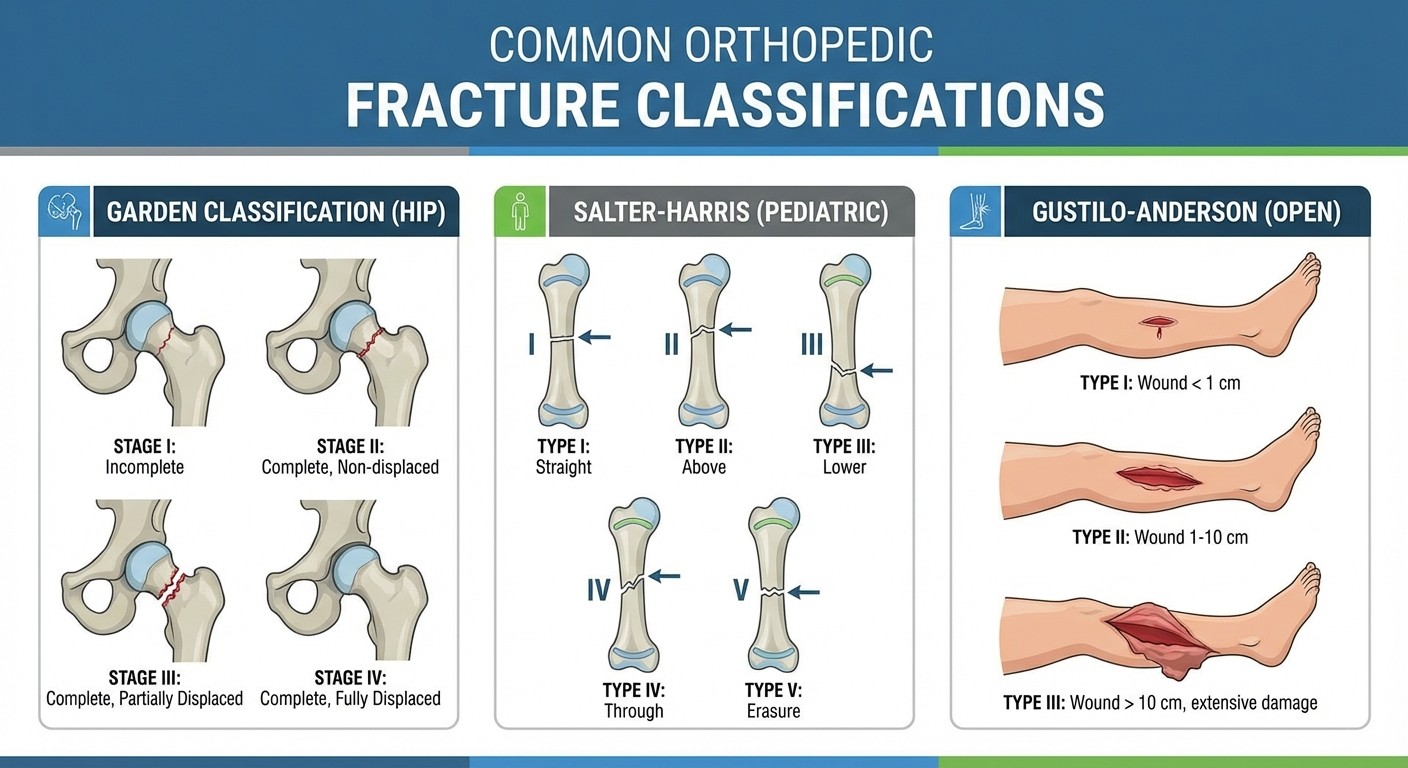
1. Garden Classification (Femoral Neck Fractures)
Garden 1: Incomplete, impacted
Garden 2: Complete, undisplaced
Garden 3: Complete, partially displaced
Garden 4: Complete, totally displaced
Clinical decision: Garden 1-2 in young patients get screw fixation. Garden 3-4 in elderly get hip replacement.
2. Salter-Harris Classification (Growth Plate Injuries)
Remember: "Straight Across, Above, beLow, Through, Ram"
Type 1: Straight across physis
Type 2: Above physis (through metaphysis)
Type 3: beLow physis (through epiphysis)
Type 4: Through everything (metaphysis + physis + epiphysis)
Type 5: Ram/crush injury
3. Gustilo-Anderson Classification (Open Fractures)
Grade 1: <1cm wound, minimal contamination
Grade 2: 1-10cm wound, moderate contamination
Grade 3A: >10cm wound, adequate soft tissue coverage
Grade 3B: >10cm wound, inadequate soft tissue coverage
Grade 3C: Any open fracture with arterial injury
4. AO/Weber Classification (Ankle Fractures)
Based on fibular fracture level relative to syndesmosis:
Type A: Below syndesmosis
Type B: At syndesmosis level
Type C: Above syndesmosis (unstable)
5. Gartland Classification (Supracondylar Fractures)
Type 1: Undisplaced
Type 2: Displaced with intact posterior cortex
Type 3: Completely displaced
When studying classifications, use the Probe game to test instant recognition of X-ray patterns — way more effective than passive reading.
Study Strategy: From Foundations to Pattern Recognition
Phase 1: Build Your Foundation (Weeks 1-2)
Start with anatomy and basic pathology. But dont get stuck memorizing muscle origins and insertions. Focus on clinically relevant anatomy:
Joint movements and muscles tested in physical exams
Nerve distributions that affect motor and sensory testing
Blood supply patterns that determine fracture healing
Use orthopedic biomechanics lessons to understand why certain fractures happen and heal the way they do.
Phase 2: Master Classifications (Weeks 2-3)
Dont just memorize — understand the clinical implications. Each classification system exists because it predicts treatment and prognosis. Create mental algorithms:
For any fracture case:
1. What's the mechanism of injury?
2. Which classification applies?
3. What does this grade/type predict about treatment?
4. What complications should I watch for?
Phase 3: Clinical Integration (Weeks 3-4)
Now connect everything through case-based learning. Take sample scenarios and work through them:
Patient age and activity level
Mechanism of injury
Physical exam findings
X-ray interpretation
Treatment decision
Expected complications
Practice this pattern recognition with orthopedics questions that simulate real NEET PG case presentations.
Image-Based Question Strategy
NEET PG orthopedics loves showing X-rays, CT scans, and clinical photos. Develop a systematic approach:
X-ray Reading Protocol
1. Check technique: Adequate penetration, proper positioning 2. Alignment: Look for breaks in normal anatomical lines 3. Bone integrity: Identify fracture lines, cortical breaks 4. Cartilage/Joint spaces: Look for narrowing or widening 5. Soft tissues: Check for swelling, foreign bodies
Common Image Patterns to Recognize
Coxa vara vs coxa valga: Neck-shaft angle changes
Scoliosis curves: Measure Cobb angle between end vertebrae
Joint space narrowing: Early sign of arthritis
Osteolytic vs osteoblastic lesions: Different metastatic patterns
When reviewing images, try explaining findings out loud. This builds the narrative thinking you'll need for exam questions. Rezzy, the AI tutor in Oncourse, can analyze your X-ray descriptions and point out missed findings.
Memory Techniques for High-Yield Facts
Mnemonics That Actually Work
VINDICATE (Differential diagnosis approach):
Vascular
Inflammatory
Neoplastic
Degenerative
Idiopathic
Congenital
Autoimmune
Traumatic
Endocrine
RICE (Acute injury management):
Rest
Ice
Compression
Elevation
5 P's of Compartment Syndrome:
Pain (out of proportion)
Pallor
Paresthesias
Pulselessness (late sign)
Paralysis (late sign)
Create visual associations for complex classifications. For Garden classification, picture a garden fence (fracture line) that can be straight (Grade 1), slightly broken (Grade 2), leaning over (Grade 3), or completely fallen down (Grade 4).
30-Day Study Schedule
Week 1: Foundation Building
Days 1-2: Basic anatomy and biomechanics
Days 3-4: Fracture healing and classification principles
Days 5-7: Trauma basics and major classifications
Week 2: System-Based Learning
Days 8-9: Upper limb injuries and surgeries
Days 10-11: Lower limb injuries and surgeries
Days 12-14: Spine pathology and pediatric orthopedics
Week 3: Clinical Integration
Days 15-16: Bone tumors and metabolic bone disease
Days 17-18: Sports medicine and arthroscopy
Days 19-21: Case-based practice and image interpretation
Week 4: Exam Preparation
Days 22-24: High-yield topic revision
Days 25-26: Mock tests and weak area identification
Days 27-30: Final review and confidence building
Track your progress with orthopedics flashcards that use spaced repetition to ensure long-term retention.
Exam Day Checklist
Must-Remember Facts for NEET PG 2026
Emergency Orthopedics:
Open fracture → Immediate irrigation and debridement
Compartment syndrome → Emergency fasciotomy
Hip dislocation → Reduce within 6 hours
Femoral neck fracture → Surgery within 24-48 hours
Age-Based Treatment Guidelines:
DDH: Pavlik harness if <6 months
Supracondylar fractures: Usually need surgery if displaced
Hip fractures in elderly: Consider replacement over fixation
Growth plate injuries: Watch for growth disturbances
Red Flag Complications:
Avascular necrosis: Hip, scaphoid, femoral head
Non-union: Scaphoid, 5th metatarsal, femoral neck
Nerve injuries: Radial nerve with humeral shaft, peroneal nerve with fibular head
Quick Recognition Patterns
Fat pad sign: Elbow effusion, suggests fracture
Sail sign: Posterior fat pad elevation on lateral elbow X-ray
Terry Thomas sign: Scapholunate dissociation gap >3mm
Double density sign: Posterior hip dislocation
Common Mistakes to Avoid
1. Over-focusing on rare conditions
Skip zebra diagnoses. NEET PG tests common presentations of common conditions, not rare syndromes that appear once in medical school.
2. Memorizing without understanding
Classifications exist for clinical decision-making. If you cant explain why a classification matters for treatment, you dont really know it.
3. Ignoring biomechanics
Many orthopedic concepts make sense when you understand forces and leverage. Fracture patterns, implant choices, and rehabilitation all follow biomechanical principles.
4. Neglecting pediatric differences
Children arent small adults. Growth plates, remodeling potential, and treatment approaches differ significantly. Dont assume adult principles apply.
Practice Resources and Tools
High-yield practice comes from case-based questions that mirror NEET PG format. Focus on:
Multi-step reasoning questions
Image interpretation with clinical correlation
Treatment algorithm decision points
Complication recognition and management
Use active recall methods like the Probe game to test instant recognition of fracture patterns. Quick image identification builds the pattern matching you need for time-pressured exams.
For complex topics like biomechanics or surgical approaches, Rezzy AI can walk through step-by-step reasoning and help identify gaps in understanding.
Frequently Asked Questions
How many orthopedics questions appear in NEET PG?
NEET PG typically includes 12-15 orthopedics questions worth 52-65 marks total. That's roughly 3% of the total exam, making it a medium-yield subject worth focused preparation.
Which fracture classifications are most important for NEET PG?
Garden (femoral neck), Salter-Harris (growth plate), Gustilo-Anderson (open fractures), Weber (ankle), and Gartland (supracondylar) appear most frequently. Master these five first before moving to specialty classifications.
How much time should I spend on orthopedics preparation?
Allocate 2-3 weeks of focused study time. Orthopedics builds on anatomy knowledge, so ensure basic musculoskeletal anatomy is solid before diving into pathology and treatments.
Are image-based questions common in NEET PG orthopedics?
Yes, expect 40-50% of orthopedics questions to include X-rays, CT scans, or clinical photos. Develop systematic image interpretation skills rather than trying to memorize specific images.
Should I memorize all muscle attachments for orthopedics?
No. Focus on clinically relevant anatomy: muscles tested in physical exams, nerve distributions affecting function, and anatomical landmarks visible on imaging. Skip detailed origin-insertion memorization.
How do I approach case-based orthopedics questions?
Use a systematic approach: patient age/mechanism → physical exam findings → imaging interpretation → classification application → treatment selection → complication awareness. Practice this workflow until it becomes automatic.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.