
Professional Medical Practice — MCQs

On this page
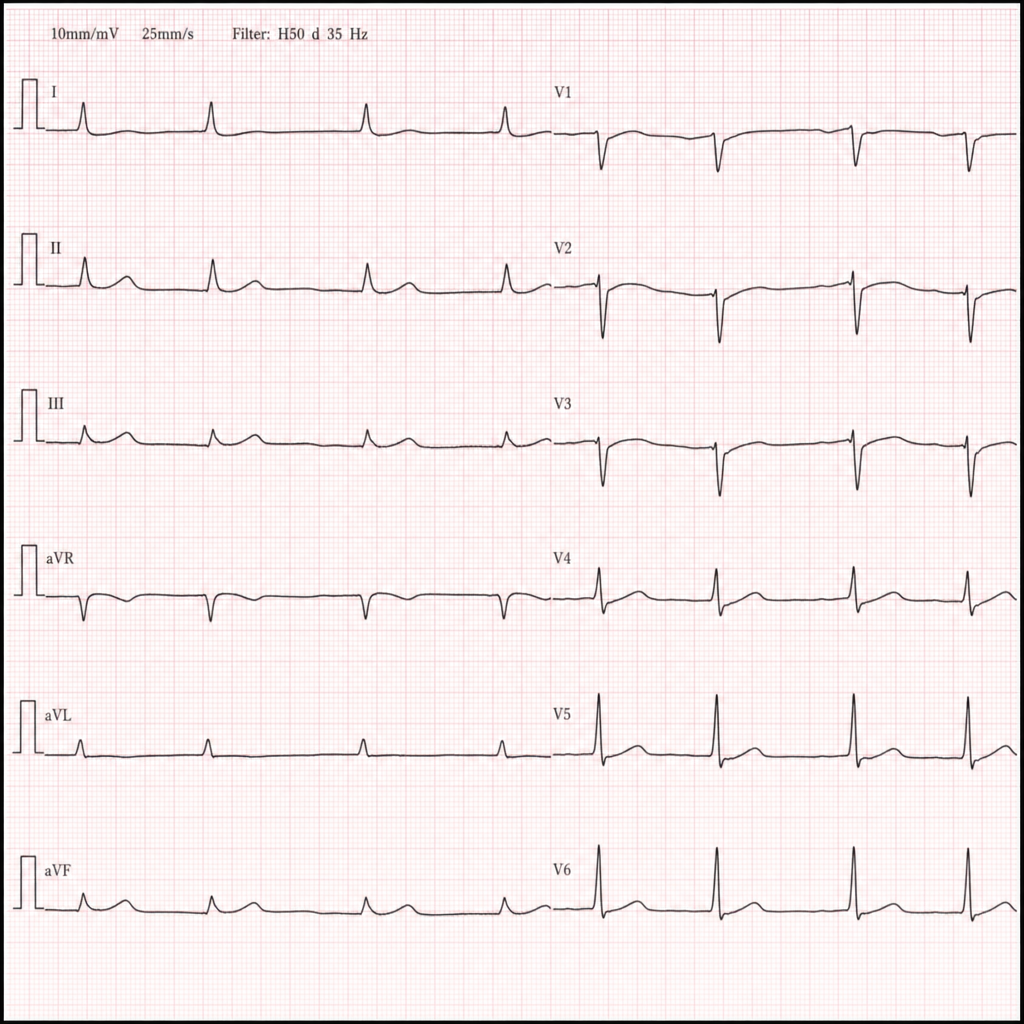
A homeless man is brought to the emergency department in January after being found unresponsive in a park. He is bradycardic and minimally responsive. A 12-lead ECG is obtained (Image 1). Which of the following is the most likely life-threatening arrhythmia if this patient's core temperature is not corrected?
A junior resident discovers that a senior consultant has been ordering unnecessary investigations for personal financial gain. After informal discussion is ignored, what is the most appropriate next step according to professional ethics?
A pharmaceutical company offers a physician free international conference registration and accommodation in exchange for prescribing their new antihypertensive drug. The drug is more expensive than equally effective alternatives. Analyze the ethical implications.
What is the primary purpose of obtaining informed consent in medical practice?
According to the Medical Council of India regulations, what is the mandatory time period for maintaining medical records in a hospital?
Which one of the following is NOT an electronic information site in surgery?
Which of the following is an example of placebo?
What does the term 'Status epilepticus' refer to in medical terminology?
Practice by Chapter
Medical Ethics and Professionalism
Practice Questions
Doctor-Patient Relationship
Practice Questions
Legal Aspects of Medical Practice
Practice Questions
Evidence-Based Medicine
Practice Questions
Healthcare Systems and Delivery
Practice Questions
Quality Improvement and Patient Safety
Practice Questions
Healthcare Economics
Practice Questions
Cross-Cultural Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app