NEET PG GIT Pharmacology Glossary 2026: PPIs, Antiemetics, H. pylori Regimens, Prokinetics and Antacids
Master GIT pharmacology for NEET PG 2026 with high-yield drug mechanisms, side effects, clinical applications, and MCQ mnemonics. Complete guide to PPIs, antiemetics, H. pylori regimens, prokinetics and antacids.
NEET PG GIT Pharmacology Glossary 2026: PPIs, Antiemetics, H. pylori Regimens, Prokinetics and Antacids
You're 3 months into NEET PG prep and GIT pharmacology feels like memorizing a phone book. PPIs, H2 blockers, prokinetics, antiemetics - 200+ drugs with overlapping mechanisms and side effects that blur together during late-night study sessions. Here's the truth: NEET PG tests pattern recognition, not rote memorization.
This glossary breaks down every high-yield GIT drug you'll see in NEET PG 2026 and INICET. We'll cover mechanisms that actually matter for MCQs, side effects they love to test, and the mnemonics that stick when you're under exam pressure. No fluff, just the drugs and concepts that show up in 80% of GIT pharmacology questions.
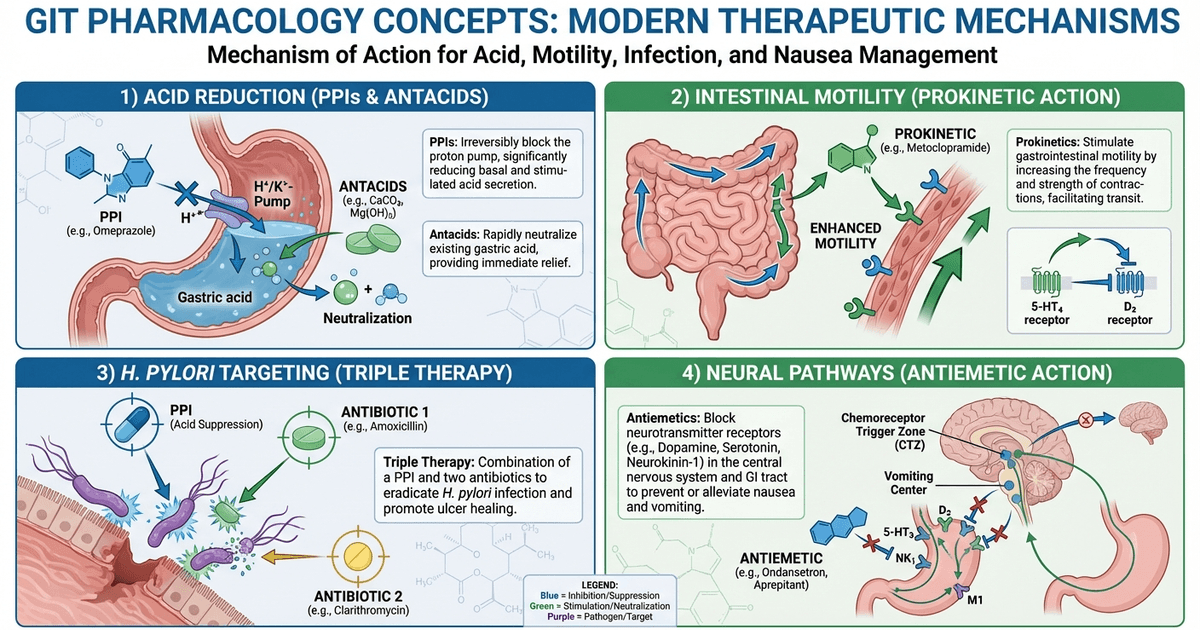
Proton Pump Inhibitors (PPIs): The Acid Suppression Masters
PPIs irreversibly inhibit H+/K+-ATPase pumps in parietal cells, achieving 90-95% acid suppression. They need acid activation to work, which is why they're taken 30 minutes before meals when acid production peaks.
High-Yield PPI Facts
Mechanism: Irreversible inhibition of proton pumps → 24-72 hour effect even after single dose Duration: Acid suppression lasts until new pumps are synthesized (3-5 days for complete recovery) First-line for: GERD, peptic ulcers, H. pylori eradication, Zollinger-Ellison syndrome
Drug | Dose | Key Points | NEET PG Favorites |
|---|---|---|---|
Omeprazole | 20-40 mg OD | First PPI, CYP2C19 metabolism | Drug interactions with warfarin, clopidogrel |
Esomeprazole | 20-40 mg OD | S-isomer of omeprazole, better bioavailability | IV formulation available |
Pantoprazole | 40 mg OD | Least drug interactions | Safest in cardiac patients |
Lansoprazole | 15-30 mg OD | Fastest onset | First-choice in elderly |
Rabeprazole | 20 mg OD | Minimal CYP metabolism | Least affected by genetic polymorphisms |
PPI Side Effects (MCQ Favorites)
Chronic use complications:
Hypomagnesemia → seizures, arrhythmias (test every 3 months on long-term therapy)
Vitamin B12 deficiency → megaloblastic anemia after 2+ years
Increased fracture risk → hip, spine, wrist (especially >65 years)
C. difficile infections → altered gut microbiome
Renal injury → acute interstitial nephritis (rare but serious)
Mnemonic: "PPIs HARM" → Pneumonia risk, Poor B12 absorption, Increased fractures, Hypomagnesemia, Acute nephritis, Rebound hyperacidity, Microbiome changes
When memorizing drug interactions, Oncourse's Synapses mnemonic engine automatically generates visual memory hooks for complex pharmacology associations - like linking omeprazole's CYP2C19 interaction to warfarin bleeding risks through memorable story chains.
PPI Clinical Pearls
Rebound hyperacidity: Occurs after stopping long-term PPIs due to gastrin-induced parietal cell hyperplasia. Taper gradually over 4-8 weeks. Drug interactions: Omeprazole inhibits CYP2C19 → reduces clopidogrel effectiveness and increases warfarin levels. Pantoprazole has minimal interactions. H. pylori resistance: PPI resistance doesn't exist - bacterial resistance is to antibiotics, not acid suppression.
H2 Receptor Antagonists: The Backup Acid Blockers
H2 blockers competitively inhibit histamine at parietal cell H2 receptors, achieving 70-80% acid suppression with 6-12 hour duration.
H2 Blocker Comparison
Drug | Potency | Key Feature | Main Side Effect |
|---|---|---|---|
Cimetidine | 1x | First H2 blocker, most interactions | Gynecomastia, anti-androgenic effects |
Ranitidine | 4x | Most prescribed (withdrawn 2019) | NDMA contamination issue |
Famotidine | 20x | Most potent, least interactions | Safest profile |
Nizatidine | 4x | No hepatic metabolism | Minimal drug interactions |
Mnemonic: "CRFN" for potency → Cimetidine (1x), Ranitidine (4x), Famotidine (20x), Nizatidine (4x)
H2 Blocker Clinical Points
Tolerance: Develops within 2-4 weeks due to receptor upregulation. Not seen with PPIs. Cimetidine specifics: Inhibits multiple CYP enzymes → increases levels of warfarin, phenytoin, theophylline. Anti-androgenic effects → gynecomastia in men, galactorrhea in women. Current status: Ranitidine withdrawn globally due to NDMA (carcinogenic) contamination. Famotidine is now first-choice H2 blocker.
Antacids: The Immediate Relief Agents
Antacids directly neutralize gastric acid, providing rapid symptom relief in 2-5 minutes but short duration (30-60 minutes).
Antacid Categories
Aluminum-based:
Aluminum hydroxide: Constipating, binds phosphate → hypophosphatemia
Best for: Hyperphosphatemia in CKD patients
Side effects: Constipation, phosphate depletion, CNS toxicity in renal failure
Magnesium-based:
Magnesium hydroxide: Laxative effect, rapid neutralization
Best for: Patients with constipation
Side effects: Diarrhea, hypermagnesemia in renal failure
Calcium-based:
Calcium carbonate: Most potent neutralizer, calcium source
Best for: Osteoporosis prevention with acid suppression
Side effects: Rebound hyperacidity, milk-alkali syndrome, constipation
Sodium bicarbonate:
Immediate action: Fastest onset, shortest duration
Best for: Acute heartburn relief
Side effects: Sodium overload, metabolic alkalosis, rebound hyperacidity
Mnemonic: "AMCS" for antacid effects → Aluminum Constipates, Magnesium Makes loose stools, Calcium Causes rebound, Sodium Supplies alkalosis
Antacid Drug Interactions
Absorption interference: Separate administration by 2 hours from:
Iron supplements (reduced absorption)
Tetracyclines (chelation)
Fluoroquinolones (chelation)
Ketoconazole (needs acid for absorption)
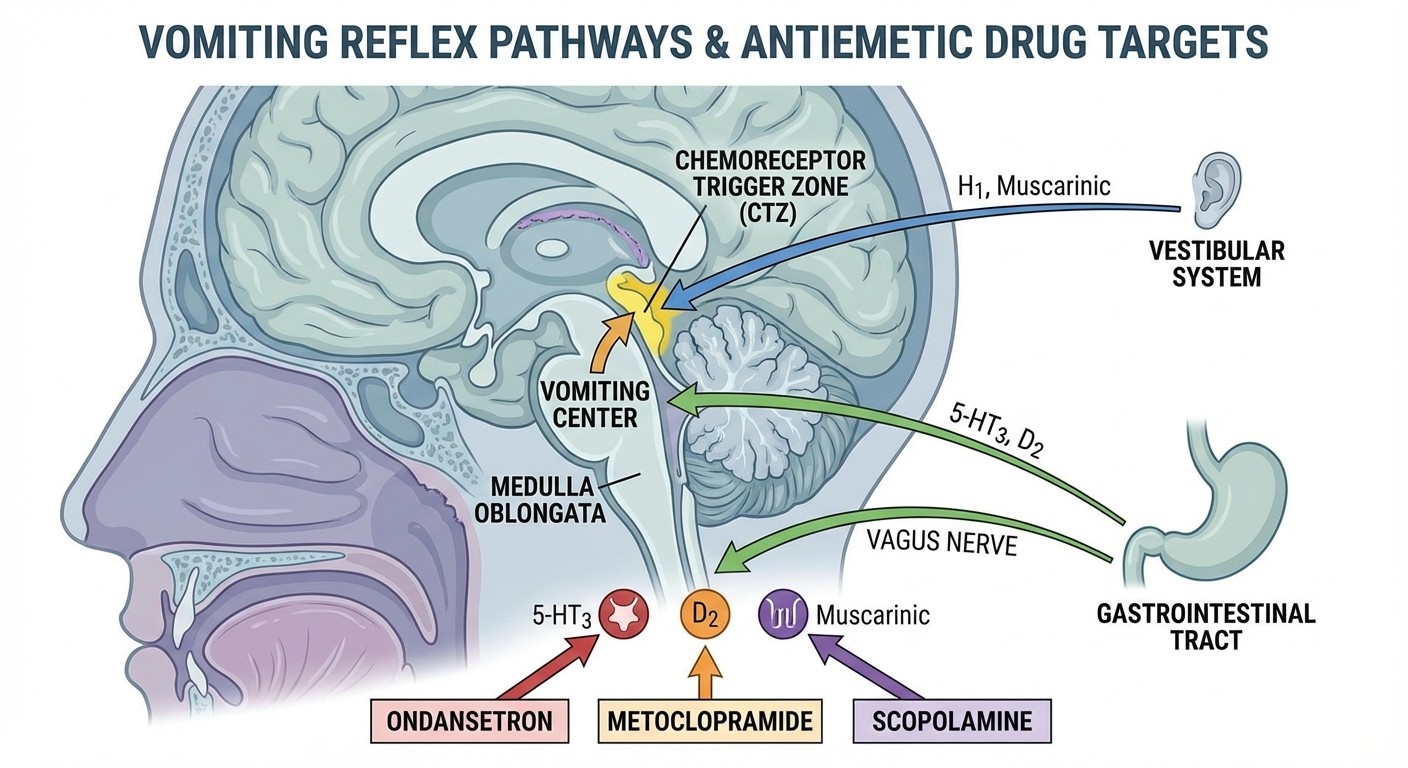
Antiemetics: The Nausea Controllers
Antiemetics target different pathways in the vomiting reflex. NEET PG tests mechanism-based drug selection for specific causes of nausea.
Antiemetic Mechanisms and Drugs
5-HT3 Antagonists (Setrons):
Ondansetron: First-line for chemotherapy-induced nausea, post-op nausea
Mechanism: Block serotonin receptors in CTZ and vagal afferents
Dose: 4-8 mg IV/PO, can repeat every 4-6 hours
Side effects: Headache, constipation, QT prolongation
NEET PG favorite: Drug of choice for cisplatin-induced emesis
Dopamine Antagonists:
Metoclopramide: D2 receptor blocker, also prokinetic
Mechanism: Blocks D2 receptors in CTZ + increases gastric motility
Dose: 10 mg TDS before meals
Side effects: Extrapyramidal symptoms, tardive dyskinesia, prolactin elevation
Contraindications: GI obstruction, pheochromocytoma
Antihistamines:
Promethazine: H1 blocker with strong sedative effects
Mechanism: Blocks histamine and muscarinic receptors
Best for: Motion sickness, pregnancy-related nausea
Side effects: Sedation, dry mouth, blurred vision
Anticholinergics:
Scopolamine: Muscarinic antagonist, transdermal patch
Mechanism: Blocks muscarinic receptors in vestibular system
Best for: Motion sickness prevention
Duration: 72-hour patch application
Antiemetic Drug Selection by Cause
Cause of Nausea | First-line Drug | Alternative | Mechanism |
|---|---|---|---|
Chemotherapy | Ondansetron | Metoclopramide | 5-HT3 blockade |
Post-operative | Ondansetron | Promethazine | CTZ inhibition |
Motion sickness | Scopolamine | Promethazine | Vestibular blockade |
Pregnancy | Promethazine | Metoclopramide | H1 antagonism |
Gastroparesis | Metoclopramide | Domperidone | Prokinetic + D2 block |
Mnemonic: "STAMP" for antiemetic selection → Setrons for Surgery/chemo, Transdermal scopolamine for Travel, Antihistamines for All-day sickness, Metoclopramide for Motility issues, Promethazine for Pregnancy
H. pylori Eradication Regimens
H. pylori resistance patterns change annually, making current regimens crucial for NEET PG 2026. Standard triple therapy success rates have dropped to 70-80% due to clarithromycin resistance.
First-line Regimens (2026 Guidelines)
Standard Triple Therapy (when clarithromycin resistance <15%):
PPI (omeprazole 20 mg BD) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
Duration: 14 days
Success rate: 70-80% (declining due to resistance)
Quadruple Therapy (first-line in high-resistance areas):
Bismuth 525 mg QID + Metronidazole 250 mg QID + Tetracycline 500 mg QID + PPI BD
Duration: 10-14 days
Success rate: 85-90%
Sequential Therapy:
Days 1-5: PPI + Amoxicillin 1 g BD
Days 6-10: PPI + Clarithromycin 500 mg BD + Metronidazole 400 mg BD
Success rate: 80-85%
Second-line Regimens
After first-line failure:
Levofloxacin-based: PPI + Levofloxacin 500 mg OD + Amoxicillin 1 g BD (10 days)
Rifabutin-based: PPI + Rifabutin 300 mg OD + Amoxicillin 1 g BD (10 days)
Mnemonic: "PAC MAN" for standard triple → PPI + Amoxicillin + Clarithromycin eats MANy pylori bacteria
H. pylori Resistance Patterns (India 2026)
Clarithromycin: 25-30% (increasing annually)
Metronidazole: 70-80% (varies by region)
Amoxicillin: <5% (rare)
Tetracycline: <5% (rare)
Levofloxacin: 15-20% (emerging)
When tackling complex H. pylori regimens, Rezzy AI can instantly explain why certain combinations work better in different resistance scenarios - like why bismuth quadruple therapy outperforms triple therapy when clarithromycin resistance exceeds 15%.
Prokinetic Agents: The Motility Enhancers
Prokinetics increase GI motility by enhancing cholinergic neurotransmission or blocking dopamine receptors that inhibit motility.
Major Prokinetic Drugs
Metoclopramide:
Mechanism: D2 antagonist + 5-HT4 agonist → increased ACh release
Indications: Gastroparesis, GERD, post-op ileus
Dose: 10 mg TDS, 30 minutes before meals
Side effects: EPS (10%), tardive dyskinesia, galactorrhea, QT prolongation
Black box warning: Risk of tardive dyskinesia with >3 months use
Domperidone:
Mechanism: Peripheral D2 antagonist (doesn't cross blood-brain barrier)
Indications: Gastroparesis, functional dyspepsia
Dose: 10 mg TDS before meals
Advantages: No EPS, safe in elderly
Side effects: Cardiac arrhythmias (high doses), hyperprolactinemia
Mosapride:
Mechanism: Selective 5-HT4 agonist
Indications: Functional dyspepsia, constipation-predominant IBS
Dose: 5 mg TDS
Advantages: No dopaminergic effects, minimal side effects
Prucalopride:
Mechanism: High-affinity 5-HT4 agonist
Indications: Chronic constipation in women
Dose: 2 mg OD
Advantages: Once-daily dosing, effective in severe cases
Prokinetic Selection Guide
Condition | First-line | Alternative | Avoid |
|---|---|---|---|
Gastroparesis | Metoclopramide | Domperidone | Anticholinergics |
Functional dyspepsia | Domperidone | Mosapride | High-dose metoclopramide |
Chronic constipation | Prucalopride | Mosapride | Metoclopramide |
Elderly patients | Domperidone | Mosapride | Metoclopramide |
Mnemonic: "DMMP" for prokinetics → Domperidone (Doesn't cross BBB), Metoclopramide (Many side effects), Mosapride (Minimal problems), Prucalopride (Perfect for women)
High-Yield MCQ Mnemonics
These mnemonics target the exact pattern NEET PG uses to test GIT pharmacology:
PPI Mnemonic Masterclass
"OMEPRAZOLE PLANS":
Onset delayed (needs acid activation)
Mechanism: irreversible H+/K+-ATPase block
Effect lasts 24-72 hours
Peptric ulcer healing 90%
Rebound hyperacidity on stopping
Alkaline environment increases drug absorption
Zollinger-Ellison syndrome treatment
Osteoporosis risk (long-term)
Lead to B12 deficiency
Enhances clopidogrel metabolism (omeprazole specifically)
Pneumonia risk increased Low magnesium (hypomagnesemia) Acute interstitial nephritis Needs gastric acid for activation Safest PPI in pregnancy (omeprazole)
Antiemetic Mechanism Memory Tool
"DOVES FLY" for antiemetic targets:
D2 receptors → Metoclopramide, Domperidone
Ondansetron → 5-HT3 receptors
Vestibular → Scopolamine (muscarinic)
Emetic center → Promethazine (H1)
Serotonin → Ondansetron
First-line chemo → Ondansetron Levo-mepromazine → D2 + multiple receptors Yesterday's choice → Chlorpromazine (now second-line)
H. pylori Triple Therapy Memory Hook
"POLICEMAN ARRESTS CRIMINALS":
POliceman = PPI + Omega (twice daily)
ARRESTS = Amoxicillin Repeated doses
CRIMINALS = Clarithromycin
For resistance: "METRO POLICE":
METRO = Metronidazole replaces clarithromycin
POLICE = POliceman (PPI) + Levofloxacin + In Cases of Emerged resistance
Drug Interactions and Contraindications
Understanding GIT drug interactions prevents dangerous combinations and optimizes therapy.
Critical PPI Interactions
CYP2C19 substrates affected by omeprazole:
Clopidogrel: Reduced effectiveness → increased CV events
Warfarin: Increased levels → bleeding risk
Phenytoin: Increased levels → toxicity signs
Safe alternatives: Pantoprazole or rabeprazole have minimal CYP interactions.
Metoclopramide Contraindications
Absolute:
GI obstruction (increases motility against blockage)
Pheochromocytoma (can trigger hypertensive crisis)
Known tardive dyskinesia
Parkinson's disease (worsens symptoms)
Relative:
Age >65 years (increased EPS risk)
Renal failure (drug accumulation)
Cardiac arrhythmias (QT prolongation)
Antacid Spacing Requirements
Separate by 2 hours from:
Iron supplements (chelation reduces absorption)
Tetracyclines (chelation forms inactive complexes)
Fluoroquinolones (reduced bioavailability by 50-90%)
Ketoconazole (needs gastric acid for dissolution)
Clinical Application Scenarios
These scenarios mirror NEET PG question patterns:
Scenario 1: Post-operative Nausea
Patient: 45-year-old female, post-cholecystectomy, severe nausea and vomiting First-line: Ondansetron 4 mg IV Why: 5-HT3 antagonists are most effective for post-operative nausea Alternative: Promethazine if ondansetron contraindicated
Scenario 2: Diabetic Gastroparesis
Patient: 50-year-old diabetic male with early satiety, bloating, vomiting undigested food First-line: Metoclopramide 10 mg TDS before meals Monitoring: Watch for EPS, especially in elderly Alternative: Domperidone if EPS occurs
Scenario 3: H. pylori in High-Resistance Area
Patient: 40-year-old male with peptic ulcer, lives in area with 30% clarithromycin resistance First-line: Bismuth quadruple therapy (14 days) Components: Bismuth + Metronidazole + Tetracycline + PPI Success rate: 85-90% vs 70% with standard triple therapy
When working through complex clinical scenarios like these, practice questions focused on GIT pharmacology help identify the exact decision points NEET PG tests - like choosing bismuth quadruple over triple therapy based on local resistance patterns.
Side Effect Spotting for MCQs
NEET PG loves testing side effect recognition. Here are the high-yield patterns:
Classic PPI Side Effects (Long-term Use)
Scenario: "A 65-year-old patient on omeprazole for 3 years presents with..."
Bone fractures → Hip/spine/wrist (mechanism: reduced calcium absorption)
Megaloblastic anemia → B12 deficiency (mechanism: requires gastric acid for B12 release)
Tetany/seizures → Hypomagnesemia (mechanism: reduced Mg2+ absorption)
Pneumonia → Altered gastric pH allows bacterial overgrowth
Metoclopramide Toxicity Red Flags
Early signs: Restlessness, anxiety, facial spasms Late signs: Tardive dyskinesia (irreversible) High-risk groups: Elderly, prolonged use >3 months Treatment: Stop drug immediately, consider benztropine for acute EPS
Antacid Metabolic Effects
Aluminum hydroxide → Constipation, phosphate depletion Magnesium hydroxide → Diarrhea, hypermagnesemia (renal failure) Calcium carbonate → Rebound hyperacidity, milk-alkali syndrome Sodium bicarbonate → Metabolic alkalosis, fluid retention
Frequently Asked Questions
What's the difference between PPIs and H2 blockers for peptic ulcer healing?
PPIs achieve 90-95% acid suppression and heal 90% of duodenal ulcers in 4 weeks. H2 blockers achieve 70-80% suppression and heal 70% of ulcers in 6-8 weeks. PPIs are first-line because they provide faster, more complete healing with once-daily dosing.
When do you use domperidone over metoclopramide?
Use domperidone in elderly patients, those at risk for extrapyramidal side effects, or when long-term prokinetic therapy is needed. Domperidone doesn't cross the blood-brain barrier, so it causes minimal neurological side effects but maintains equal prokinetic efficacy.
How do you remember which antiemetic to use for chemotherapy vs motion sickness?
Think mechanism: Chemotherapy causes nausea via serotonin release from gut → use 5-HT3 antagonists (ondansetron). Motion sickness involves vestibular system → use anticholinergics (scopolamine) or antihistamines (promethazine).
Why has H. pylori triple therapy success rate declined?
Clarithromycin resistance has increased from <10% to 25-30% in India over the past decade. When resistance exceeds 15-20%, triple therapy success drops below 80%. This is why current guidelines recommend bismuth quadruple therapy as first-line in high-resistance areas.
What's the most important PPI drug interaction to remember?
Omeprazole inhibits CYP2C19, reducing clopidogrel's effectiveness and increasing warfarin levels. Use pantoprazole or rabeprazole in patients on these medications, as they have minimal CYP interactions.
When do PPIs cause rebound hyperacidity and how do you prevent it?
Rebound occurs after stopping long-term PPIs (>8 weeks) due to gastrin-induced parietal cell hyperplasia. Prevent by tapering over 4-8 weeks or switching to H2 blockers before discontinuation. The rebound typically resolves in 1-2 weeks after complete discontinuation.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS