Back
How to Study Biostatistics and PSM for NEET PG 2026: Sensitivity, Specificity, PPV, NPV and High-Yield MCQ Strategy
Master biostatistics for NEET PG 2026 with this complete guide to sensitivity, specificity, PPV, NPV calculations and high-yield MCQ strategies. Get the 30-day study plan.

How to Study Biostatistics and PSM for NEET PG 2026: Sensitivity, Specificity, PPV, NPV and High-Yield MCQ Strategy
You are staring at a biostatistics MCQ and the numbers are swimming. Disease prevalence 15%, sensitivity 85%, specificity 92% — calculate the PPV. Your brain goes blank.
This happens to 80% of NEET PG aspirants. Biostatistics and PSM (Preventive and Social Medicine) account for 15-20 questions in NEET PG, yet most students treat them as "scoring subjects" without understanding the core concepts. The result? Easy marks lost to calculation errors and concept confusion.
Here's the truth: biostatistics in NEET PG isnt about complex statistical analysis. Its about understanding 4 key concepts so well that you can solve any sensitivity-specificity question in under 60 seconds. This guide breaks down exactly how to master these concepts and develop a foolproof MCQ strategy.
Understanding the 2x2 Contingency Table: Your Foundation
Every biostatistics question in NEET PG starts with a 2x2 contingency table. Master this, and youve solved 70% of biostat problems.
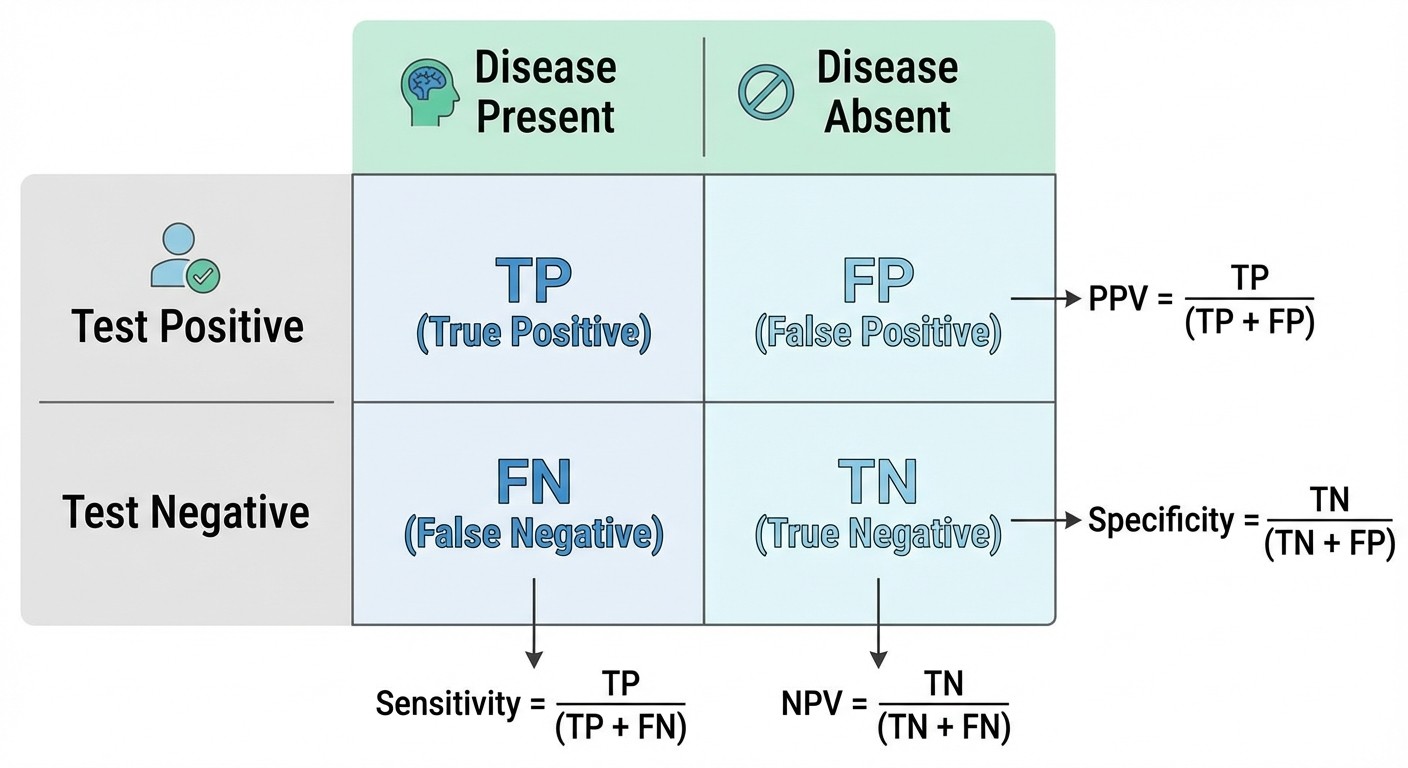
The table has 4 cells:
True Positive (TP): Test positive, disease present
False Positive (FP): Test positive, disease absent
True Negative (TN): Test negative, disease absent
False Negative (FN): Test negative, disease present
Here's the key insight most students miss: every biostat concept flows from these 4 numbers. Memorize this table structure first, then the formulas become logical instead of random.
Practice tip: Draw this table from memory 10 times daily until its automatic. When you see any biostat question, immediately draw the table and fill in the given numbers. This single habit will prevent 90% of calculation mistakes.
The Big Four: Sensitivity, Specificity, PPV, NPV
Sensitivity (True Positive Rate)
Formula: TP / (TP + FN) Memory trick: "SN-out" — Sensitivity rules out disease when Negative What it means: Among people with disease, what percentage test positive?
High sensitivity = few false negatives = good screening test. A 95% sensitive test misses only 5% of diseased patients.
Common NEET PG trap: Students confuse sensitivity with accuracy. Sensitivity only looks at diseased patients, not the total population.
Specificity (True Negative Rate)
Formula: TN / (TN + FP) Memory trick: "SP-in" — Specificity rules in disease when Positive What it means: Among healthy people, what percentage test negative?
High specificity = few false positives = good confirmatory test. A 98% specific test falsely labels only 2% of healthy people as diseased.
Positive Predictive Value (PPV)
Formula: TP / (TP + FP) Memory trick: "Of all positive tests, how many are truly positive?" Key insight: PPV depends heavily on disease prevalence
This is where most students stumble. PPV isnt fixed like sensitivity — it changes with prevalence. In high-prevalence populations, even average tests have high PPV. In low-prevalence screening, even excellent tests have poor PPV.
Negative Predictive Value (NPV)
Formula: TN / (TN + FN) Memory trick: "Of all negative tests, how many are truly negative?" Key insight: NPV is high when disease prevalence is low
NPV behaves opposite to PPV. In rare diseases, negative results are almost always correct because most people dont have the disease anyway.
The Prevalence Effect: Why Context Matters
Heres the concept that separates toppers from average scorers: prevalence dramatically affects PPV and NPV, but never touches sensitivity or specificity.
Example scenario (classic NEET PG style):
Test sensitivity: 90%
Test specificity: 95%
Population A prevalence: 50%
Population B prevalence: 1%
In Population A (high prevalence), PPV = ~95%
In Population B (low prevalence), PPV = ~15%
Same test, completely different usefulness. This is why screening tests need ultra-high specificity, while diagnostic tests in sick patients can accept lower specificity.
The mental model: Sensitivity and specificity are intrinsic test properties. PPV and NPV depend on who youre testing. When you master this distinction, biostat questions become pattern recognition instead of calculation nightmares.
High-Yield Calculation Shortcuts
The 1000-Patient Method
Instead of working with percentages, assume 1000 patients and work with whole numbers. This eliminates decimal errors and makes calculations visual.
Example: Sensitivity 80%, Specificity 90%, Prevalence 10%
Step 1: 1000 patients total
Step 2: 100 have disease (10%), 900 dont have disease (90%)
Step 3: Of 100 diseased, 80 test positive (sensitivity 80%), 20 test negative
Step 4: Of 900 healthy, 90 test positive (false positive rate 10%), 810 test negative
Step 5: Calculate PPV = 80/(80+90) = 80/170 = 47%
This method works for any combination and takes 30 seconds once youre fluent. Practice this with biostatistics MCQs until its second nature.
The Quick Prevalence Check
Before calculating PPV/NPV, ask: "Is prevalence high or low?"
High prevalence (>20%): PPV will be decent, NPV might be lower
Low prevalence (<5%): PPV will be poor, NPV will be excellent
This gut check prevents absurd answers. If you calculate PPV as 95% for a 1% prevalence scenario, you know something went wrong.
ROC Curves and Likelihood Ratios: The Advanced Concepts
NEET PG increasingly tests ROC (Receiver Operating Characteristic) curves and likelihood ratios. These seem complex but follow simple rules.
ROC Curves
The ROC curve plots sensitivity vs (1-specificity) for different cut-off values. Key facts for NEET PG:
Perfect test: Curve goes straight up then straight right (area = 1.0)
Useless test: Diagonal line (area = 0.5)
Good test: Area under curve >0.8
Excellent test: Area under curve >0.9
Most questions ask you to identify the better test (higher AUC) or the optimal cut-off point (closest to upper left corner).
Likelihood Ratios
Positive LR = Sensitivity / (1-Specificity) Negative LR = (1-Sensitivity) / Specificity
Memory shortcuts:
LR+ >10: Strong evidence for disease
LR+ 5-10: Moderate evidence for disease
LR+ 2-5: Weak evidence for disease
LR+ <2: Minimal evidence for disease
Negative LR works in reverse (lower is better for ruling out).
The beauty of likelihood ratios: they dont change with prevalence. A test with LR+ of 20 provides strong evidence regardless of population. Use this for questions that compare test performance across different settings.
Common NEET PG Question Patterns
Pattern 1: The Direct Calculation
"A screening test has sensitivity 85% and specificity 92%. In a population with disease prevalence 8%, what is the PPV?"
Approach: Use the 1000-patient method, calculate step-by-step.
Pattern 2: The Comparison Question
"Which test is better for screening: Test A (Sens 95%, Spec 85%) or Test B (Sens 80%, Spec 98%)?"
Key insight: Screening prioritizes specificity to minimize false positives. Test B is better despite lower sensitivity.
Pattern 3: The Prevalence Shift
"The same test is used in two populations with different disease prevalence. Which statement is correct about PPV and NPV?"
Answer template: PPV increases with prevalence, NPV decreases with prevalence. Sensitivity and specificity remain constant.
Pattern 4: The Clinical Scenario
"A doctor wants to rule out MI in chest pain patients. Which test characteristic is most important?"
Logic: To rule out, you need high sensitivity (minimize false negatives). A highly sensitive test, when negative, effectively rules out disease.
Memory Techniques That Actually Work
The SNOUT and SPIN Method
SNOUT: SeNsitive test, when Negative, rules OUT disease
SPIN: SPecific test, when Positive, rules IN disease
This helps choose the right test for clinical scenarios. Emergency screening needs SNOUT tests. Confirmatory diagnosis needs SPIN tests.
The Fraction Visualization
Instead of memorizing formulas, visualize what youre calculating:
Sensitivity: "Of diseased people, how many test positive?"
Specificity: "Of healthy people, how many test negative?"
PPV: "Of positive tests, how many are truly positive?"
NPV: "Of negative tests, how many are truly negative?"
The question word ("how many") tells you what goes in numerator and denominator.
The Mnemonic Building
Create your own memory devices using Oncourse's Synapses feature, which helps build personalized mnemonics for complex biostat concepts. The interactive format lets you associate visual cues with formulas until they become automatic.
The 30-Day Biostatistics Mastery Plan
Week 1: Foundation Building
Day 1-3: Master the 2x2 table structure
Day 4-5: Practice basic sensitivity/specificity calculations
Day 6-7: Understand prevalence effects on PPV/NPV
Daily target: 10 basic MCQs using the 1000-patient method
Week 2: Pattern Recognition
Day 8-10: Identify high-yield question patterns
Day 11-12: Practice ROC curve interpretation
Day 13-14: Master likelihood ratio calculations
Daily target: 15 mixed MCQs, focus on question pattern identification
Week 3: Speed and Accuracy
Day 15-17: Timed practice sessions (1 minute per question)
Day 18-19: Common error analysis and correction
Day 20-21: Advanced concepts (confidence intervals, hypothesis testing)
Daily target: 20 MCQs under time pressure
Week 4: Integration and Review
Day 22-24: Mixed biostat + clinical integration questions
Day 25-26: Previous year NEET PG biostat analysis
Day 27-28: Weak area targeted practice
Daily target: 25 mixed questions, emphasizing clinical application
Use biostatistics flashcards for daily formula review and biostatistics lessons for concept reinforcement.
Integration with Clinical Subjects
Biostatistics isnt isolated. NEET PG increasingly tests biostat within clinical contexts:
Medicine Integration
Diagnostic test evaluation for cardiac markers
Screening guidelines for diabetes and hypertension
Risk factor analysis for metabolic syndrome
Surgery Integration
Surgical outcome prediction models
Complication rate calculations
Preoperative risk stratification tools
OBG Integration
Prenatal screening test accuracy
Birth rate and fertility statistics
Maternal mortality ratio calculations
Pediatrics Integration
Growth chart interpretation (percentiles, Z-scores)
Vaccination efficacy studies
Developmental milestone statistics
The strategy: when reviewing clinical subjects, note any statistical concepts. Create mental links between biostat principles and clinical applications. This dual approach reinforces both subjects simultaneously.
Technology-Enhanced Learning
Modern biostat preparation benefits from interactive tools that make abstract concepts concrete:
Practice with adaptive MCQ platforms that adjust difficulty based on your performance. Tools like Oncourse's biostatistics questions use AI to identify your weak areas and provide targeted practice.
Use spaced repetition for formula retention. The key insight: understanding beats memorization, but both are necessary. Build conceptual understanding first, then use spaced repetition to make calculations automatic.
Try simulation-based learning where you manipulate test parameters and see how sensitivity, specificity, PPV, and NPV change in real-time. This builds intuitive understanding that pure calculation practice cant provide.
Common Mistakes to Avoid
Mistake 1: Formula Cramming Without Understanding
Students memorize "PPV = TP/(TP+FP)" without understanding what it represents. When the question format changes slightly, they panic.
Solution: Always start with the conceptual meaning, then derive the formula.
Mistake 2: Ignoring Prevalence Effects
Treating PPV and NPV as fixed test characteristics like sensitivity and specificity.
Solution: Before any PPV/NPV calculation, consciously note the prevalence and predict whether PPV will be high or low.
Mistake 3: Decimal Confusion
Working with percentages and getting lost in decimal calculations during time pressure.
Solution: Use the 1000-patient method consistently. Integer arithmetic is faster and more accurate under stress.
Mistake 4: Clinical Context Ignorance
Solving biostat questions mechanically without considering what the numbers mean clinically.
Solution: After every calculation, ask "Does this result make clinical sense?" A screening test with 5% PPV in a low-prevalence population is mathematically correct but clinically useless.
The PSM Integration Strategy
Biostatistics doesnt exist in isolation within NEET PG — its woven throughout PSM topics. Heres how to study them together:
Epidemiology Connection
Study designs (RCT, cohort, case-control) generate different types of statistical measures
Learn which statistical tests apply to which study designs
Understand bias and confounding in statistical terms
Health Planning Connection
Demographic indices use statistical principles
Health indicator calculations require biostat understanding
Resource allocation models use epidemiological data
Environmental Health Connection
Dose-response relationships use correlation and regression
Risk assessment models use statistical prediction
Pollution studies use hypothesis testing
The integration approach: Study PSM topics chronologically, but when statistics appear, cross-reference with core biostat principles. This creates a web of understanding rather than isolated subject boxes.
Frequently Asked Questions
What percentage of NEET PG questions come from biostatistics?
Biostatistics typically accounts for 8-12 questions out of 200 total NEET PG questions, making it roughly 4-6% of the paper. However, these questions have high accuracy rates among prepared students, making them crucial for rank optimization.
Should I focus more on sensitivity/specificity or other biostat topics?
Sensitivity, specificity, PPV, and NPV form the core of 60-70% of biostat questions. Master these first, then move to correlation, regression, and hypothesis testing. The 80/20 rule applies: 20% of topics yield 80% of marks.
How much time should I allocate daily to biostatistics during NEET PG prep?
Dedicate 30-45 minutes daily for the first month to build strong foundations. After mastery, 15-20 minutes of daily practice maintains accuracy. Biostat requires consistent practice more than intensive cramming.
Are calculator skills important for biostatistics in NEET PG?
NEET PG allows basic calculators, but most biostat calculations are designed for mental math or simple calculations. Practice the 1000-patient method and estimation techniques — they're faster than calculator dependence.
How do I improve speed in biostatistics MCQs?
Speed comes from pattern recognition, not faster calculation. Practice identifying question types instantly, then apply the appropriate shortcut method. Aim for 45-60 seconds per biostat MCQ through deliberate practice.
What's the difference between Type I and Type II errors in NEET PG context?
Type I error (α) = rejecting true null hypothesis = false positive at population level. Type II error (β) = accepting false null hypothesis = false negative at population level. NEET PG questions often test this conceptual understanding rather than calculations.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.