How to Study Immunology for NEET PG 2026: Complete High-Yield Strategy for Hypersensitivity, Autoimmune Diseases and MCQ Patterns
Master immunology for NEET PG 2026 with this complete guide covering hypersensitivity reactions, autoimmune diseases, complement system, and high-yield mnemonics. Includes exam patterns and study strategies.
How to Study Immunology for NEET PG 2026: Complete High-Yield Strategy for Hypersensitivity, Autoimmune Diseases and MCQ Patterns
You are probably staring at your immunology chapter wondering where to even begin. T cells, B cells, complement cascades, 20 different cytokines, autoantibody after autoantibody — it feels like learning a foreign language. Here is the truth: immunology scared me too until I figured out the pattern.
NEET PG 2026 will ask you 12-15 immunology questions. That is roughly 6% of your score riding on concepts that most students either skip or memorize poorly. The difference between a 620 and a 650+ score often comes down to nailing these high-yield immunology MCQs that others get wrong.
This guide cuts through the noise. After analyzing 5 years of NEET PG papers and scoring in the 99th percentile, here is exactly what shows up, how often, and the fastest way to master it. No fluff. Just the immunology that wins seats.
Why Immunology Feels Hard (And Why It Doesnt Have To Be)
Most students approach immunology like pathology — trying to understand every mechanism from first principles. That is a mistake. Immunology in NEET PG is pattern recognition disguised as mechanism understanding.
The examiners love three things:
1. Association questions: Which autoantibody goes with which disease?
2. Classification questions: Type I vs Type II vs Type III vs Type IV hypersensitivity
3. Deficiency questions: What happens when complement component X is missing?
Once you realize this, immunology becomes a structured memory game. The mechanisms matter less than knowing that anti-dsDNA means SLE, that Type II hypersensitivity uses IgG, and that C3 deficiency causes recurrent pyogenic infections.
What to Expect from Immunology in NEET PG 2026
Question Distribution (Based on Last 5 Years):
Autoimmune diseases: 4-5 questions
Hypersensitivity reactions: 3-4 questions
Immunodeficiency syndromes: 2-3 questions
Complement system: 1-2 questions
Transplant immunology: 1-2 questions
Vaccines/cytokines: 1-2 questions
Favorite Question Formats:
"A 25-year-old female presents with butterfly rash and anti-dsDNA positive. Diagnosis?"
"Type III hypersensitivity is mediated by which mechanism?"
"A child with recurrent Neisseria infections has deficiency of which complement component?"
The pattern is clear: they want you to match clinical presentations with immunologic mechanisms. Study accordingly.
The Big 5 Subtopics to Master (Ranked by Exam Frequency)
1. Hypersensitivity Reactions (Type I-IV) — Most Tested
This is your highest-yield topic. Every NEET PG paper has 3-4 hypersensitivity questions.
Type I (Immediate, IgE-mediated)
Mechanism: IgE bound to mast cells → degranulation
Clinical: Anaphylaxis, allergic rhinitis, asthma, food allergies
Mediators: Histamine, leukotrienes, prostaglandins
Timeline: Minutes
Type II (Cytotoxic, IgG/IgM-mediated)
Mechanism: Antibodies against cell surface antigens → complement activation
Clinical: ABO incompatibility, autoimmune hemolytic anemia, Goodpasture syndrome
Key feature: Direct cell destruction
Timeline: Hours
Type III (Immune Complex-mediated)
Mechanism: Antibody-antigen complexes deposit in tissues
Clinical: SLE, rheumatoid arthritis, serum sickness, Arthus reaction
Key feature: Vasculitis, glomerulonephritis
Timeline: Hours to days
Type IV (Delayed-type, T-cell mediated)
Mechanism: Th1 cells activate macrophages
Clinical: Contact dermatitis, tuberculin test, transplant rejection
Key feature: No antibodies involved
Timeline: 24-72 hours
Mnemonic: "ACID"
Anaphylaxis (Type I)
Cytotoxic (Type II)
Complex-mediated (Type III)
Delayed (Type IV)
Practice with our immunology lessons that break down each type with clinical examples and MCQ patterns.
2. Autoimmune Diseases — Antibody-Disease Pairings
This section wins or loses 4-5 marks every year. The key is memorizing which antibody predicts which disease.
High-Yield Autoantibodies:
Antibody | Disease | Additional Info |
|---|---|---|
Anti-dsDNA | SLE | Specific for SLE, correlates with nephritis |
Anti-Smith | SLE | Most specific for SLE |
Anti-Ro/SSA | Sjögren syndrome | Also causes neonatal lupus |
Anti-La/SSB | Sjögren syndrome | More specific than Anti-Ro |
Anti-centromere | Limited scleroderma | CREST syndrome |
Anti-Scl70 | Diffuse scleroderma | Poor prognosis |
c-ANCA | Granulomatosis with polyangiitis | Wegener granulomatosis |
p-ANCA | Microscopic polyangiitis | Also eosinophilic granulomatosis |
Anti-CCP | Rheumatoid arthritis | More specific than RF |
Anti-Jo1 | Polymyositis | Antisynthetase syndrome |
Memory Trick: Group by organ system. Kidney (anti-dsDNA, ANCA), joints (anti-CCP, RF), skin (anti-centromere, anti-Scl70), glands (anti-Ro, anti-La).
Test your antibody knowledge with targeted autoimmune disease questions that mirror NEET PG patterns.
3. Immunodeficiency Syndromes — Primary vs Secondary
NEET PG loves asking about primary immunodeficiencies because they test both immunology and pediatrics knowledge.
B-Cell Deficiencies:
Bruton agammaglobulinemia: No mature B cells, recurrent bacterial infections after 6 months
CVID: Low IgG, IgA, normal B cell count
IgA deficiency: Most common, recurrent sinopulmonary infections
T-Cell Deficiencies:
DiGeorge syndrome: Thymic aplasia, hypocalcemia, cardiac defects (22q11 deletion)
Chronic mucocutaneous candidiasis: Isolated T-cell defect against Candida
Combined Deficiencies:
SCID: No T or B cell function, death by 1 year without BMT
Wiskott-Aldrich: Thrombocytopenia + eczema + immunodeficiency
Ataxia-telangiectasia: Cerebellar ataxia + immunodeficiency + radiation sensitivity
Quick Assessment Rule:
Bacterial infections → B-cell defect
Viral/fungal infections → T-cell defect
Both → Combined defect
Memory Aid: "BAD WASteD SCID" — Bruton, Ataxia-telangiectasia, DiGeorge, Wiskott-Aldrich, SCID
Reinforce these concepts with primary immunodeficiency flashcards that use spaced repetition to lock in the key features.
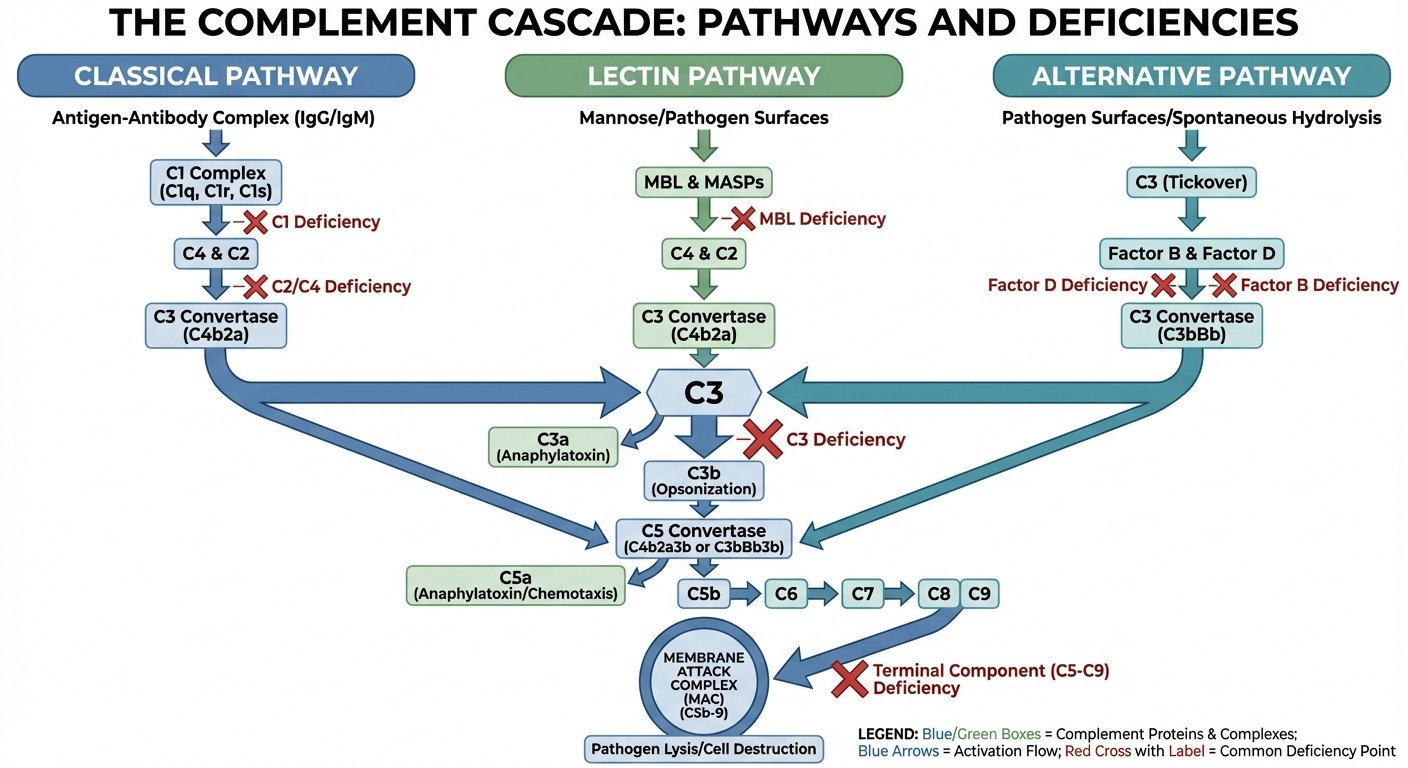
4. Complement System — Classical vs Alternative vs Lectin
The complement system appears in 1-2 questions annually. Focus on the pathways and deficiency consequences.
Three Pathways: 1. Classical: Antigen-antibody complexes → C1 → C4 → C2 → C3 2. Alternative: Microbial surfaces → Factor B → Factor D → C3 3. Lectin: Mannose-binding lectin → MASP-1/2 → C4 → C2 → C3 All paths converge at C3 → C5 → membrane attack complex (MAC) High-Yield Deficiencies:
C1, C2, C4: SLE-like syndrome (immune complex clearance defect)
C3: Severe recurrent bacterial infections (opsonization defect)
C5-C9: Recurrent Neisseria infections (MAC defect)
Factor H/I: Hemolytic uremic syndrome
Mnemonic: "Some Lupus Needs Complement"
Some = C1,C2,C4 cause SLE
Lupus = Late complement (C5-C9) causes Neisseria
Needs = No C3 = No bacteria clearing
Complement = Complement fixes everything
Study complement pathways systematically with our complement system lessons that include pathway diagrams and deficiency tables.
5. Transplant Immunology — HLA and Rejection Types
Transplant questions usually focus on HLA matching and rejection mechanisms.
HLA System:
Class I (A, B, C): On all nucleated cells, present to CD8+ T cells
Class II (DR, DQ, DP): On APCs, present to CD4+ T cells
Inheritance: Haploid from each parent, 25% chance of sibling match
Rejection Types: 1. Hyperacute (minutes-hours): Pre-formed antibodies, immediate thrombosis 2. Acute (days-weeks): T-cell mediated, responds to immunosuppression 3. Chronic (months-years): Slow fibrosis, irreversible GVHD vs Host vs Graft:
GVHD: Donor T cells attack host (bone marrow transplant)
Rejection: Host T cells attack graft (solid organ transplant)
Quick Rule: If it happens immediately = hyperacute. If it responds to steroids = acute. If it is slow and irreversible = chronic.
High-Yield Mnemonics for Each Subtopic
Hypersensitivity Types: "ACID Hippos"
Anaphylactic (Type I) - Allergy, Asthma
Cytotoxic (Type II) - Cells destroyed
Immune complex (Type III) - In tissues
Delayed (Type IV) - Days later
Autoimmune Antibodies: "SLE Drinks Sclerosis Coffee"
SLE = Smith, ss-DNA
Drinks = Diffuse scleroderma = Scl-70
Sclerosis = Sjögren = SSA/SSB (Ro/La)
Coffee = Centromere = CREST
Primary Immunodeficiencies: "BAD Kids Waste Away Seriously"
Bruton (B-cell)
Ataxia-telangiectasia (Combined)
DiGeorge (T-cell)
Wiskott-Aldrich (Combined)
SCID (Combined)
Complement Deficiencies: "Early Lupus, Late Neisseria"
Early complement (C1,C2,C4) → Lupus-like
Late complement (C5-C9) → Neisseria infections
Cytokine Functions: "I Love T-Cells Being Activated"
IL-1 = Inflammation starter
Love = IL-2 = Lymphocyte growth
T-Cells = TNF-α = Tumor necrosis
Being = IL-4 = B-cell activation
Activated = IFN-γ = Activates macrophages
Vaccines and Immunoglobulins — Passive vs Active
Active Immunization (Vaccines):
Live attenuated: MMR, varicella, rotavirus, BCG
Killed/inactivated: Polio (IPV), influenza, rabies
Toxoids: Diphtheria, tetanus
Subunit: Hepatitis B, HPV, pneumococcal
Passive Immunization (Ready-made antibodies):
Hepatitis A: Post-exposure + vaccine
Hepatitis B: High-risk exposure + vaccine
Varicella: Immunocompromised contacts
Rabies: Post-exposure + vaccine
Tetanus: Dirty wounds + toxoid
Key Rule: Passive immunization for immediate protection, active for long-term immunity.
Learn vaccine schedules and indications through our comprehensive vaccine lessons with updated 2026 guidelines.
Cytokines You MUST Know
Pro-inflammatory:
IL-1: Fever, acute phase response
IL-6: Fever, acute phase proteins
TNF-α: Shock, cachexia, apoptosis
IL-12: Drives Th1 response
IL-17: Neutrophil recruitment
Anti-inflammatory:
IL-10: Suppresses macrophages
IL-4: Drives Th2, IgE production
TGF-β: Tissue repair, fibrosis
T-cell specific:
IL-2: T-cell proliferation
IFN-γ: Macrophage activation
B-cell specific:
IL-4: Class switching to IgE
IL-5: Eosinophil activation, IgA
One-Line Memory: "1 and 6 cause Fever, 2 grows T-cells, 4 makes IgE, 5 calls Eosinophils, 10 calms Everything"
Commonly Confused Concepts
Type II vs Type III Hypersensitivity:
Type II: Antibodies attack cells directly (hemolysis)
Type III: Antibody-antigen complexes deposit in tissues (vasculitis)
SLE vs Drug-induced Lupus:
SLE: Anti-dsDNA positive, kidney involvement
Drug-induced: Anti-histone positive, no kidney involvement
SCID vs DiGeorge:
SCID: No T or B cells, infections from birth
DiGeorge: T-cell defect only, thymic aplasia + hypocalcemia
CVID vs IgA Deficiency:
CVID: Low IgG, IgA, and often IgM
IgA deficiency: Only IgA low, others normal
Primary vs Secondary Immunodeficiency:
Primary: Genetic, presents early, specific patterns
Secondary: Acquired (HIV, malnutrition, drugs), broader susceptibility
When you hit these confusing concepts, Rezzy AI can explain the mechanisms step-by-step and help you understand why one answer is better than another. Access our AI tutor for instant clarification of tricky immunology concepts.
How Oncourse AI Accelerates Your Immunology Prep
Targeted Question Bank: Our adaptive algorithm identifies which immunology subtopics you are weak in and serves more questions from those areas. Instead of random practice, you get focused drilling on hypersensitivity types or autoantibody associations where you need it most. Synapses Mnemonics: Use our Synapses flashcard game to lock in antibody-disease pairings through spaced repetition. The system tracks which associations you forget and brings them back at optimal intervals. Instant AI Explanations: When you miss a complement system question, Rezzy explains not just the right answer but why the other pathways dont fit. It is like having an immunology professor available 24/7 to clarify mechanisms. Pattern Recognition: Our question bank includes 500+ immunology MCQs modeled after NEET PG patterns. You will see the same question formats that appear on exam day, helping you recognize the triggers that point to specific answers.
Final 2-Week Immunology Revision Checklist
Week 1: Core Concepts
[ ] Memorize all autoantibody-disease pairs (use flashcards daily)
[ ] Practice 20 hypersensitivity questions daily
[ ] Review complement pathways with diagrams
[ ] Learn primary immunodeficiency features
Week 2: Pattern Recognition
[ ] Solve 50 mixed immunology MCQs daily
[ ] Review vaccine schedules and passive immunization
[ ] Practice cytokine function questions
[ ] Revise transplant rejection types
Daily Revision (Both Weeks):
Morning: 1 immunology topic + 10 MCQs
Evening: Mnemonics review + weak areas from practice
Night: Quick flashcard run through autoantibodies
Red Flags to Review Again:
Any autoantibody you cant match instantly
Complement deficiency consequences
Type III vs Type II hypersensitivity differences
Primary immunodeficiency inheritance patterns
Practice systematically with our immunology question bank that covers all high-yield topics with detailed explanations.
Frequently Asked Questions
How many immunology questions come in NEET PG 2026?
Expect 12-15 immunology questions across microbiology, pathology, medicine, and pediatrics. That is roughly 6% of your total score, making it a high-impact topic worth mastering.
Which immunology topic has the highest weightage?
Autoimmune diseases and hypersensitivity reactions account for 60-70% of immunology questions. Focus on antibody-disease associations and hypersensitivity mechanisms first.
How should I memorize autoantibody patterns?
Use spaced repetition flashcards and group antibodies by organ system. Practice daily until you can match any antibody to its disease within 3 seconds.
Is complement system important for NEET PG?
Yes, 1-2 questions appear annually. Focus on the three pathways, C3/C5 cleavage, and deficiency consequences rather than detailed biochemistry.
Should I study transplant immunology in detail?
Learn HLA basics and rejection types, but dont go deep into immunosuppressive drugs unless you are also preparing transplant surgery topics.
How do I differentiate between primary immunodeficiencies?
Focus on inheritance patterns, age of presentation, and infection types. B-cell defects cause bacterial infections, T-cell defects cause viral/fungal infections.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition flashcards, and AI explanations built specifically for NEET PG 2026. Download free on Android and iOS.