Back
FMGE Pharmacology High Yield Topics 2026: Complete Guide for Foreign Medical Graduates
Master FMGE pharmacology with this complete guide covering high-yield topics for 2026. Essential drug classes, mechanisms, and exam strategies for foreign medical graduates.

FMGE Pharmacology High Yield Topics 2026: Complete Guide for Foreign Medical Graduates
You are staring at 25-30 pharmacology questions in FMGE 2026. Each one worth the difference between clearing and repeating. Here is the thing most foreign medical graduates miss: pharmacology isnt just memorizing drug names. Its understanding receptor mechanisms, clinical applications, and side effect profiles that NBE loves to test.
After analyzing FMGE patterns from 2020-2025, certain pharmacology topics appear consistently. While anatomy gives you 40+ questions and gets all the attention, pharmacology silently determines whether you cross the finish line. The passing candidates I know didnt study every drug in Goodman & Gilman. They identified the high-yield 20% that covers 80% of exam questions.
FMGE 2026 has 300 total questions across 19 subjects. Pharmacology typically contributes 25-30 questions (roughly 8-10% weightage). But here is what makes it tricky: pharmacology questions often cross-reference with medicine, surgery, and obstetrics cases. A single CVS drug question might test mechanism, indication, contraindication, and adverse effects simultaneously.
This guide breaks down exactly what to study and what to skip. No textbook theory, no low-yield exceptions. Just the systematically tested pharmacology concepts that show up year after year.
Understanding FMGE 2026 Pharmacology Exam Pattern
FMGE pharmacology questions follow predictable patterns. NBE examiners focus on clinical pharmacology over basic mechanisms. You will see more "Which drug is contraindicated in this patient?" than "Draw the chemical structure."
Question Distribution by System:
ANS pharmacology: 4-6 questions
CVS drugs: 5-7 questions
CNS pharmacology: 4-5 questions
Chemotherapy (antibiotics/antimalarials): 6-8 questions
Endocrine pharmacology: 2-3 questions
Autacoids and anti-inflammatory: 2-3 questions
Toxicology: 2-3 questions
Common Question Formats: 1. Mechanism-based: "MOA of chloroquine against malaria" 2. Clinical application: "First-line drug for hypertensive crisis" 3. Adverse effects: "Most serious side effect of amiodarone" 4. Contraindications: "Drug avoided in pregnancy" 5. Drug interactions: "Warfarin + aspirin effect"
The key insight: FMGE tests practical drug knowledge you would need as a practicing doctor in India, not research-level pharmacology.
High-Yield General Pharmacology Concepts
Before diving into system-specific drugs, nail these foundational concepts that appear across multiple pharmacology questions.
Pharmacokinetics Essentials
Bioavailability and First-Pass Metabolism
Sublingual nitroglycerin bypasses first-pass (100% bioavailable)
Oral morphine has 30% bioavailability due to extensive first-pass
IV drugs always have 100% bioavailability
Half-Life Clinical Applications
5 half-lives for complete elimination
Digoxin (36-hour half-life) takes 7 days to reach steady state
Loading doses needed for drugs with long half-lives
When memorizing drug half-lives, the pharmacology flashcards use spaced repetition to surface the exact values at optimal review intervals.
Drug Receptor Interactions
Agonist vs Antagonist Concepts
Full agonist: maximum response possible (morphine at opioid receptors)
Partial agonist: submaximal response even at saturation (buprenorphine)
Competitive antagonist: reversible by increasing agonist (naloxone vs morphine)
Non-competitive antagonist: irreversible blockade (phenoxybenzamine)
Clinical Significance
Partial agonists have ceiling effect (safer in overdose)
Non-competitive antagonists require new receptor synthesis
Competitive antagonism follows rightward shift in dose-response curve
Tolerance and Dependence
Physical vs Psychological Dependence
Physical: withdrawal symptoms on discontinuation
Psychological: craving and drug-seeking behavior
Cross-tolerance: tolerance to one drug extends to similar drugs
High-Yield Examples
Opioid tolerance develops to analgesia but not to constipation
Benzodiazepine withdrawal can cause fatal seizures
Barbiturate tolerance involves enzyme induction
ANS Pharmacology: High-Yield Drug Classes
Autonomic nervous system pharmacology consistently yields 4-6 FMGE questions. Focus on receptor selectivity and clinical uses rather than detailed biochemistry.
Cholinergic System
Acetylcholine Receptors
Nicotinic: ligand-gated Na+/K+ channels (muscle, ganglia)
Muscarinic: G-protein coupled (M1-M5 subtypes)
Cholinesterase Inhibitors
Physostigmine: crosses blood-brain barrier, reverses atropine toxicity
Neostigmine: doesnt cross BBB, treats myasthenia gravis
Organophosphates: irreversible binding, treated with atropine + pralidoxime
The mnemonic "NEOS saves MG" (Neostigmine saves Myasthenia Gravis) helps remember the specific indication. For complex drug classifications like this, the mnemonic engine generates visual acronym chains that make cholinergic drugs stick in memory under exam pressure.
Adrenergic System
Receptor Selectivity
α1: vasoconstriction (phenylephrine)
α2: presynaptic inhibition (clonidine)
β1: cardiac stimulation (dobutamine)
β2: bronchodilation (salbutamol)
β3: lipolysis (rarely tested)
Clinical Applications by Receptor
α1 agonists: nasal decongestants, maintain BP during spinal anesthesia
α1 antagonists: BPH (tamsulosin), hypertension (doxazosin)
β1 selective blockers: heart failure (metoprolol), post-MI
β2 agonists: asthma (salbutamol), delay preterm labor (terbutaline)
High-Yield Drug Specifics
Epinephrine reversal: α-blocked epinephrine causes β2-mediated hypotension
Cocaine blocks Na+ channels AND norepinephrine reuptake
Tyramine effect: indirect sympathomimetic, dangerous with MAOIs
Neuromuscular Junction
Depolarizing vs Non-depolarizing Blockers
Succinylcholine: depolarizing, rapid onset, fasciculations
Atracurium: non-depolarizing, reversed by neostigmine
Vecuronium: non-depolarizing, liver metabolism
Clinical Considerations
Succinylcholine contraindicated in burns (hyperkalemia)
Malignant hyperthermia triggered by succinylcholine + halothane
Pseudocholinesterase deficiency prolongs succinylcholine action
CVS Pharmacology: Critical Drug Categories
Cardiovascular pharmacology contributes 5-7 questions consistently. FMGE emphasizes antihypertensives, antiarrhythmics, and anticoagulants over inotropes.
Antihypertensive Drugs
ACE Inhibitors vs ARBs
ACE inhibitors end in "-pril" (enalapril, captopril)
ARBs end in "-sartan" (losartan, valsartan)
Both reduce mortality in heart failure
ACE inhibitors cause dry cough (10-15%), ARBs dont
Calcium Channel Blockers
Dihydropyridines (amlodipine): vascular selective, ankle edema
Non-dihydropyridines (verapamil, diltiazem): cardiac effects, negative inotrope
Diuretic Classification
Loop diuretics: furosemide, inhibit Na-K-2Cl transporter
Thiazides: hydrochlorothiazide, inhibit Na-Cl transporter
K-sparing: spironolactone (aldosterone antagonist), amiloride
Practice cardiovascular pharmacology MCQs to master the clinical application scenarios that FMGE favors.
Antiarrhythmic Drugs
Vaughan Williams Classification
Class I: Na+ channel blockers (quinidine, lidocaine)
Class II: β-blockers (propranolol, metoprolol)
Class III: K+ channel blockers (amiodarone, sotalol)
Class IV: Ca2+ channel blockers (verapamil)
High-Yield Specifics
Amiodarone: most effective, multiple side effects (thyroid, pulmonary)
Lidocaine: IV only, first-line for VT during MI
Digoxin: increases vagal tone, narrow therapeutic window
Anticoagulants and Antiplatelets
Mechanism-Based Classification
Heparin: activates antithrombin III, immediate effect
Warfarin: inhibits vitamin K synthesis, delayed onset
Novel anticoagulants: direct thrombin (dabigatran) or factor Xa inhibitors
Antiplatelet Agents
Aspirin: irreversibly inhibits COX-1, affects bleeding time
Clopidogrel: ADP receptor antagonist, alternative to aspirin
Prasugrel: stronger ADP antagonist, higher bleeding risk
Clinical Monitoring
Heparin: aPTT (activated partial thromboplastin time)
Warfarin: INR (international normalized ratio)
Novel anticoagulants: no routine monitoring needed
CNS Pharmacology: Essential Drug Classes
Central nervous system drugs contribute 4-5 FMGE questions, focusing on sedative-hypnotics, antiepileptics, and antipsychotics.
Sedative-Hypnotics
Benzodiazepine Mechanism
Enhance GABA-A receptor function (dont activate directly)
Increase frequency of chloride channel opening
Flumazenil is specific competitive antagonist
Duration-Based Classification
Ultra-short: triazolam (anesthesia)
Short: midazolam (procedures)
Intermediate: lorazepam (anxiety)
Long: diazepam (seizures)
Clinical Applications
Status epilepticus: IV diazepam or lorazepam
Alcohol withdrawal: chlordiazepoxide or diazepam
Anesthesia premedication: midazolam
Antiepileptic Drugs
Mechanism Categories
Na+ channel blockers: phenytoin, carbamazepine
GABA enhancers: phenobarbital, valproate
Ca2+ channel blockers: ethosuximide (absence seizures)
Drug-Specific Profiles
Phenytoin: zero-order kinetics, gingival hyperplasia
Carbamazepine: autoinduction of metabolism, diplopia
Valproate: broad spectrum, teratogenic (neural tube defects)
Ethosuximide: absence seizures only, minimal side effects
When a student gets an antiepileptic MCQ wrong, the explanation chat provides instant Socratic breakdown of why phenytoin affects Na+ channels while ethosuximide targets T-type Ca2+ channels.
Antipsychotic Drugs
Typical vs Atypical Classification
Typical: block D2 receptors, cause extrapyramidal side effects
Atypical: block D2 + 5-HT2A, lower EPS risk
High-Yield Examples
Haloperidol: typical, high potency, severe EPS
Chlorpromazine: typical, low potency, sedating
Risperidone: atypical, prolactin elevation
Clozapine: atypical, agranulocytosis risk
Side Effect Profiles
Extrapyramidal: dystonia, parkinsonism, tardive dyskinesia
Metabolic: weight gain, diabetes (atypicals)
Cardiac: QT prolongation (haloperidol, thioridazine)
Chemotherapy: High-Yield Antimicrobials
Antimicrobial chemotherapy typically contributes 6-8 questions to FMGE. Focus on mechanism, spectrum, and resistance patterns rather than chemical structures.
Antibiotic Classification by Mechanism
Cell Wall Synthesis Inhibitors
β-lactams: penicillins, cephalosporins, carbapenems
Vancomycin: binds D-ala-D-ala peptide sequences
Mechanism: bactericidal against growing bacteria
Protein Synthesis Inhibitors
30S inhibitors: streptomycin, gentamicin, tetracyclines
50S inhibitors: chloramphenicol, erythromycin, clindamycin
Generally bacteriostatic (except aminoglycosides)
Study antimicrobial questions to master the clinical scenarios where mechanism knowledge determines the correct choice.
β-Lactam Antibiotics
Penicillin Categories
Natural: penicillin G (IV), penicillin V (oral)
Anti-staphylococcal: methicillin, nafcillin
Broad-spectrum: ampicillin, amoxicillin
Anti-pseudomonal: piperacillin, ticarcillin
Cephalosporin Generations
1st generation: gram-positive coverage (cefazolin)
2nd generation: improved gram-negative (cefuroxime)
3rd generation: excellent gram-negative, crosses BBB (ceftriaxone)
4th generation: broad spectrum including Pseudomonas (cefepime)
Antimalarial Drugs
Chloroquine vs Primaquine
Chloroquine: blood schizonticide, resistance widespread
Primaquine: tissue schizonticide, radical cure for P. vivax
Mefloquine: chloroquine-resistant areas, neuropsychiatric effects
Artemisinin: rapid action, always used in combination
Clinical Applications
Uncomplicated P. falciparum: artemisinin combinations
P. vivax radical cure: chloroquine + primaquine
Severe malaria: IV artesunate
Prophylaxis: depends on resistance pattern in travel area
Antitubercular Drugs
First-Line Anti-TB Drugs
Isoniazid: inhibits mycolic acid synthesis, hepatotoxicity
Rifampin: RNA polymerase inhibitor, orange discoloration
Ethambutol: damages optic nerve, test visual acuity
Pyrazinamide: requires acidic pH, hyperuricemia
Standard Treatment Regimen
Intensive phase (2 months): isoniazid + rifampin + ethambutol + pyrazinamide
Continuation phase (4 months): isoniazid + rifampin
DOT (directly observed therapy) recommended
Autacoids and Anti-Inflammatory Drugs
This section contributes 2-3 FMGE questions annually, focusing on NSAIDs and antihistamines.
NSAID Classification and Mechanisms
COX Selectivity
Non-selective: aspirin, ibuprofen, diclofenac
COX-2 selective: celecoxib, rofecoxib (withdrawn)
COX-1 preferential: low-dose aspirin (antiplatelet)
Mechanism-Based Side Effects
GI toxicity: COX-1 inhibition reduces protective prostaglandins
Renal toxicity: reduced PGE2 and PGI2 in kidney
Cardiovascular risk: COX-2 selectivity may increase thrombosis
When learning NSAID side effect profiles, the daily mnemonic challenge presents acronym puzzles like "NSAID GI Risk = No Stomach Acid In Duodenum Gets Inflamed Readily" to reinforce the gastroprotective role of prostaglandins.
Antihistamines
H1 vs H2 Receptor Antagonists
H1 antagonists: treat allergic reactions (diphenhydramine, loratadine)
H2 antagonists: reduce gastric acid (ranitidine, famotidine)
First vs Second Generation H1 Antagonists
First generation: sedating, cross blood-brain barrier
Second generation: non-sedating, selective peripheral action
Corticosteroids
Anti-Inflammatory Mechanism
Inhibit phospholipase A2 via lipocortin
Reduce arachidonic acid release
Decrease prostaglandin and leukotriene synthesis
Clinical Uses vs Side Effects
Short-term: inflammation, allergy, asthma exacerbations
Long-term complications: osteoporosis, diabetes, infections
Withdrawal: must be gradual to prevent adrenal insufficiency
Endocrine Pharmacology
Endocrine drugs contribute 2-3 FMGE questions, emphasizing diabetes medications and thyroid drugs.
Antidiabetic Drugs
Insulin Types by Duration
Rapid-acting: lispro, aspart (onset 5-15 minutes)
Short-acting: regular insulin (onset 30 minutes)
Intermediate: NPH insulin (onset 2-4 hours)
Long-acting: glargine, detemir (24-hour duration)
Oral Antidiabetic Mechanisms
Sulfonylureas: stimulate insulin release (glyburide, glipizide)
Metformin: decreases hepatic glucose production
Thiazolidinediones: increase insulin sensitivity
DPP-4 inhibitors: prolong incretin action
Clinical Considerations
Metformin: lactic acidosis risk with kidney disease
Sulfonylureas: hypoglycemia and weight gain
Insulin: only option for type 1 diabetes
Thyroid Medications
Antithyroid Drugs
Methimazole: blocks thyroid peroxidase, preferred agent
Propylthiouracil: blocks TPO + peripheral T4→T3 conversion
Radioactive iodine: permanent ablation of thyroid tissue
Clinical Applications
Graves disease: methimazole or radioactive iodine
Thyroid storm: PTU + propranolol + steroids
Pregnancy: PTU preferred (methimazole teratogenic)
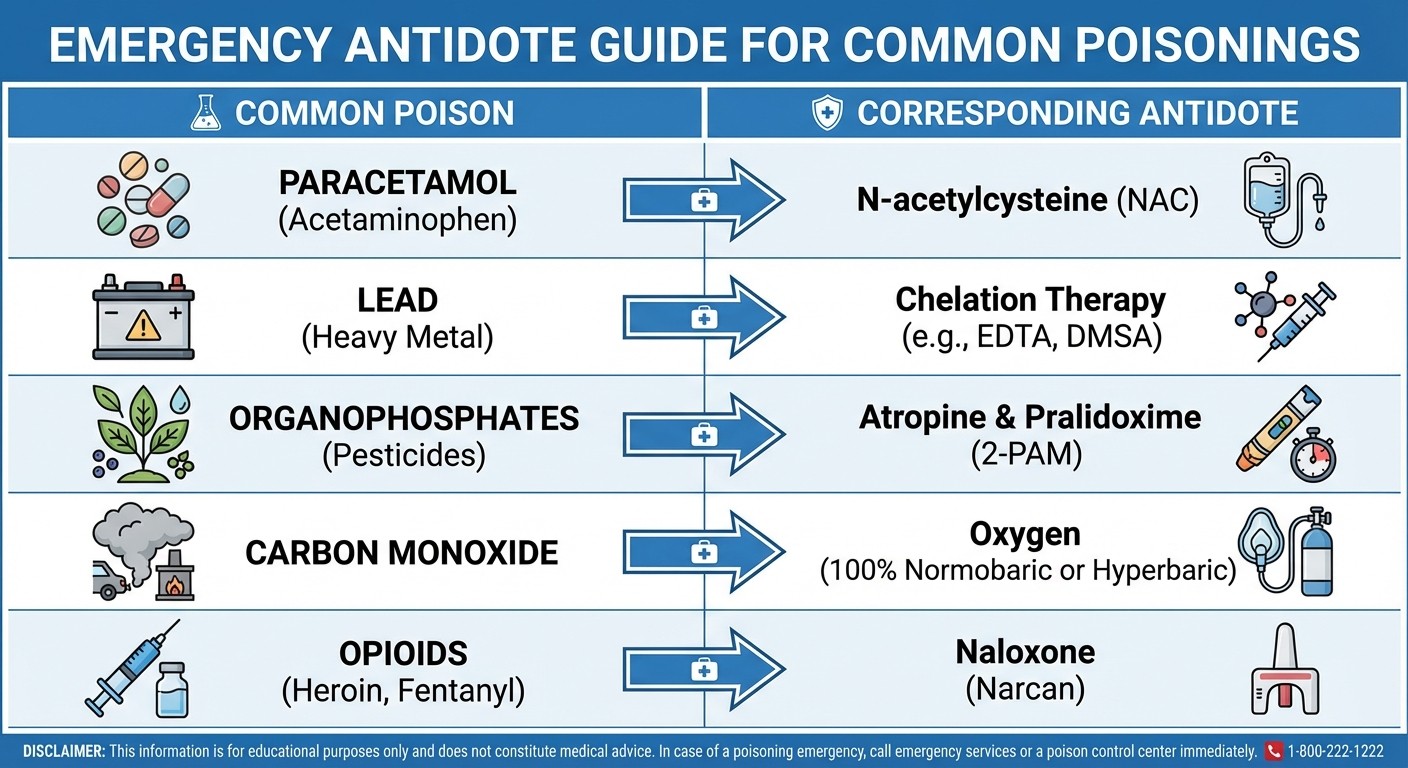
Toxicology: High-Yield Poisonings
Toxicology contributes 2-3 questions focusing on common poisonings and antidotes.
Organophosphate Poisoning
Mechanism and Symptoms
Irreversible cholinesterase inhibition
Muscarinic effects: SLUDGE syndrome
Nicotinic effects: fasciculations, paralysis
Treatment Protocol
Atropine: blocks muscarinic effects (give until atropinization)
Pralidoxime: reactivates cholinesterase (within 24 hours)
Supportive: airway management, seizure control
Specific Antidotes
Poison | Antidote | Mechanism |
|---|---|---|
Paracetamol | N-acetylcysteine | Replenishes glutathione |
Iron | Deferoxamine | Chelation |
Lead | Dimercaprol, EDTA | Chelation |
Cyanide | Hydroxocobalamin | Forms cyanocobalamin |
Methanol | Ethanol, Fomepizole | Competitive inhibition |
Digoxin | Digoxin-specific Fab | Binds free digoxin |
Smart Study Strategies for FMGE Pharmacology
Here is how to systematically tackle pharmacology without getting overwhelmed by the sheer volume of drugs and mechanisms.
The 3-Pass System
Pass 1: Core Mechanisms (Week 1-2)
Study drug classifications by mechanism
Focus on prototype drugs for each class
Build the framework before adding details
Pass 2: Clinical Applications (Week 3-4)
Learn indications and contraindications
Practice mechanism-to-clinical reasoning
Review pharmacology lessons systematically
Pass 3: Exam-Specific Details (Week 5-6)
Side effects and drug interactions
Dose modifications in special populations
High-yield facts and mnemonics
Memory Techniques for Drug Names
Pattern Recognition
β-blockers end in "-olol" (propranolol, metoprolol)
ACE inhibitors end in "-pril" (enalapril, lisinopril)
ARBs end in "-sartan" (losartan, irbesartan)
Mechanism-Based Grouping
Instead of learning individual drugs, group by mechanism:
All drugs that block Na+ channels together
All drugs that enhance GABA function together
All drugs that inhibit prostaglandin synthesis together
After completing a pharmacology topic, create flashcards from the lesson content and let the spaced repetition algorithm schedule optimal review times.
Avoiding Common FMGE Pitfalls
Drug Name Confusion
Atropine (antimuscarinic) vs Atracurium (neuromuscular blocker)
Atenolol (β-blocker) vs Albuterol (β-agonist)
Quinidine (antiarrhythmic) vs Quinine (antimalarial)
Mechanism Oversimplification
Dont memorize "aspirin prevents heart attacks" without understanding COX-1 inhibition
Learn why certain side effects occur, not just what they are
Connect pharmacology to pathophysiology you already know
Clinical Context Neglect
FMGE tests drugs in clinical scenarios, not isolation
A hypertension question might test ACE inhibitor contraindications
An asthma question might test β-agonist selectivity
Rapid Review: Must-Know Drug Lists
Life-Saving Drug Knowledge
Anaphylaxis: epinephrine IM, corticosteroids, H1 + H2 antihistamines
Status epilepticus: IV diazepam/lorazepam, then phenytoin
Opioid overdose: naloxone IV, may need repeated doses
Organophosphate poisoning: atropine + pralidoxime
Paracetamol toxicity: N-acetylcysteine within 8 hours
Drug Interactions to Remember
Warfarin + aspirin: increased bleeding risk
ACE inhibitors + potassium supplements: hyperkalemia
Digoxin + quinidine: digoxin toxicity (displacement from protein binding)
Phenytoin + other enzyme inducers: accelerated metabolism
MAOIs + tyramine-rich foods: hypertensive crisis
Pregnancy Safety Categories
Category A: folic acid, levothyroxine
Category B: penicillins, cephalosporins, insulin
Category C: most drugs (risk-benefit analysis needed)
Category D: phenytoin, valproate, lithium
Category X: warfarin, isotretinoin, thalidomide
Frequently Asked Questions
How many pharmacology questions appear in FMGE 2026?
Pharmacology contributes 25-30 questions out of 300 total questions in FMGE 2026. This represents roughly 8-10% of the exam weightage. However, pharmacology knowledge also helps with clinical questions in medicine, surgery, and other subjects.
Which pharmacology topics have highest weightage in FMGE?
Chemotherapy (especially antibiotics) and cardiovascular pharmacology consistently yield the most questions. ANS drugs and CNS pharmacology also appear frequently. Focus your energy on these four areas before studying endocrine or specialized drug classes.
Should I memorize drug doses for FMGE?
FMGE rarely tests specific drug doses. Focus on mechanisms, indications, contraindications, and side effects instead. The few dose-related questions usually involve concepts like loading doses or dose adjustments in renal failure, not memorizing specific numbers.
How do I remember drug classifications effectively?
Use pattern recognition and mechanism-based grouping. Most drug names follow predictable patterns (β-blockers end in "-olol", ACE inhibitors end in "-pril"). Group drugs by mechanism rather than trying to memorize individual drug properties.
What is the best way to practice FMGE pharmacology MCQs?
Practice systematically by topic rather than random questions. Start with general pharmacology questions, then move to ANS drugs, CVS pharmacology, and so on. This builds your knowledge progressively.
How important is toxicology for FMGE pharmacology?
Toxicology typically contributes 2-3 questions focusing on common poisonings and antidotes. Learn the major antidote-poison pairs (atropine for organophosphates, N-acetylcysteine for paracetamol, naloxone for opioids) and you will cover most scenarios.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for FMGE. Download free on Android and iOS.