
Autonomic Nervous System Drugs — MCQs

On this page
A 28-year-old man develops descending flaccid paralysis, diplopia and dysphagia after eating improperly canned food. Another patient develops rapid paralysis after eating puffer fish. Which of the following correctly matches the mechanism of action?
Which of the following drugs possesses similar cycloplegic action and is a more potent mydriatic than atropine?
Which beta-blocker possesses an additional alpha-blocking property?
Which of the following drugs binds only with the anionic site of cholinesterase?
Atracurium is primarily eliminated by which mechanism?
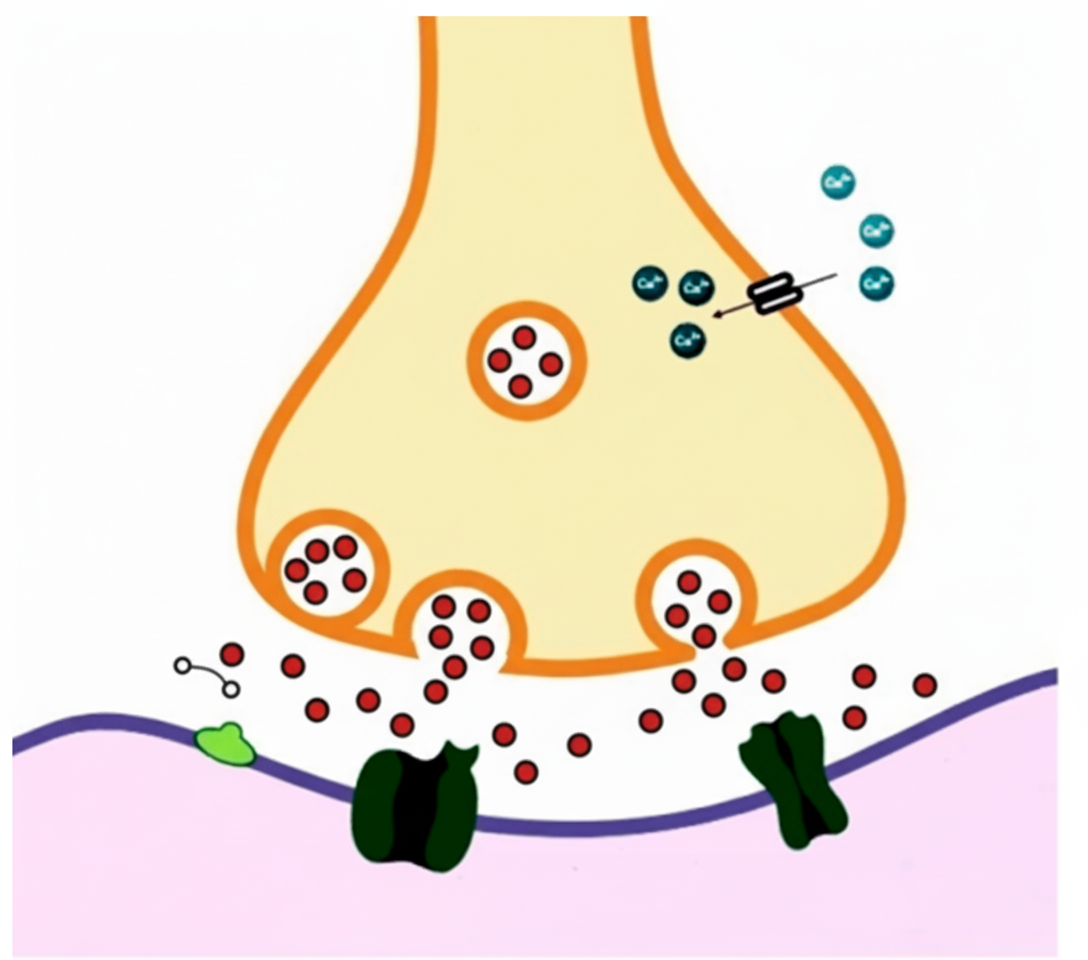
A 30-year-old theatre actress developed facial wrinkles. The treating physician advised local injections of a drug indicated in cervical dystonia, spastic disorders like cerebral palsy, and prophylaxis of migraine. The physician warned of potential side effects including dry mouth and blurred vision. The actress identified the drug's site of action as depicted in the accompanying figure. Which of the following drugs is being described?
Propranolol is contraindicated in diabetes mellitus because it:
A 68-year-old male with hypertension presents for annual examination. On review of systems, he reports urinary hesitancy and nocturia. His examination reveals a nontender but enlarged prostate without nodules. His blood pressure logs and clinic readings show average values of 150/80 mm Hg. Which medication offer treatment of hypertension and prostatic symptoms?
Which is a depolarizing skeletal muscle relaxant?
In atropine instillation, all are seen except:
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app