
Cardiology — MCQs

On this page
A 35-year-old patient presents to the emergency department with sudden onset severe headache and dizziness following a motor vehicle accident. After initial assessment, the patient is sent for an urgent CT scan of the head. CT scan reveals a mild hypodensity in the left cerebellum. What is the most likely etiology/cause?
A 67-year-old woman is brought to the emergency department by her caretakers for a change in behavior. The patient lives in a nursing home and was noted to have abnormal behavior, urinary incontinence, and trouble walking. The patient has been admitted to the hospital before for what seems to be negligence from her caretakers. Laboratory values are ordered as seen below. Serum: Na+: 120 mEq/L Cl-: 98 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.2 mg/dL Urinalysis is notable for bacteruria without pyuria or nitrates. Physical exam is notable for a confused woman who is unable to answer questions appropriately. She states she has no pain or symptoms and is not sure why she is here. She thinks the year is 1982. Which of the following complications could be seen with treatment of this patient?
A 77-year-old male presents to the emergency department because of shortness of breath and chest discomfort. The patient states his ability to withstand activity has steadily declined, and most recently he has been unable to climb more than one flight of stairs without having to stop to catch his breath. On physical exam, the patient has a harsh crescendo-decrescendo systolic murmur heard over the right sternal border, with radiation to his carotids. Which of the following additional findings are most likely in this patient?
A plain CT scan of the patient's head is performed immediately and shows no evidence of hemorrhage. His temperature is 37.1°C (98.8°F), pulse is 101/min and blood pressure is 174/102 mm Hg. Which of the following is the most appropriate next step in management?
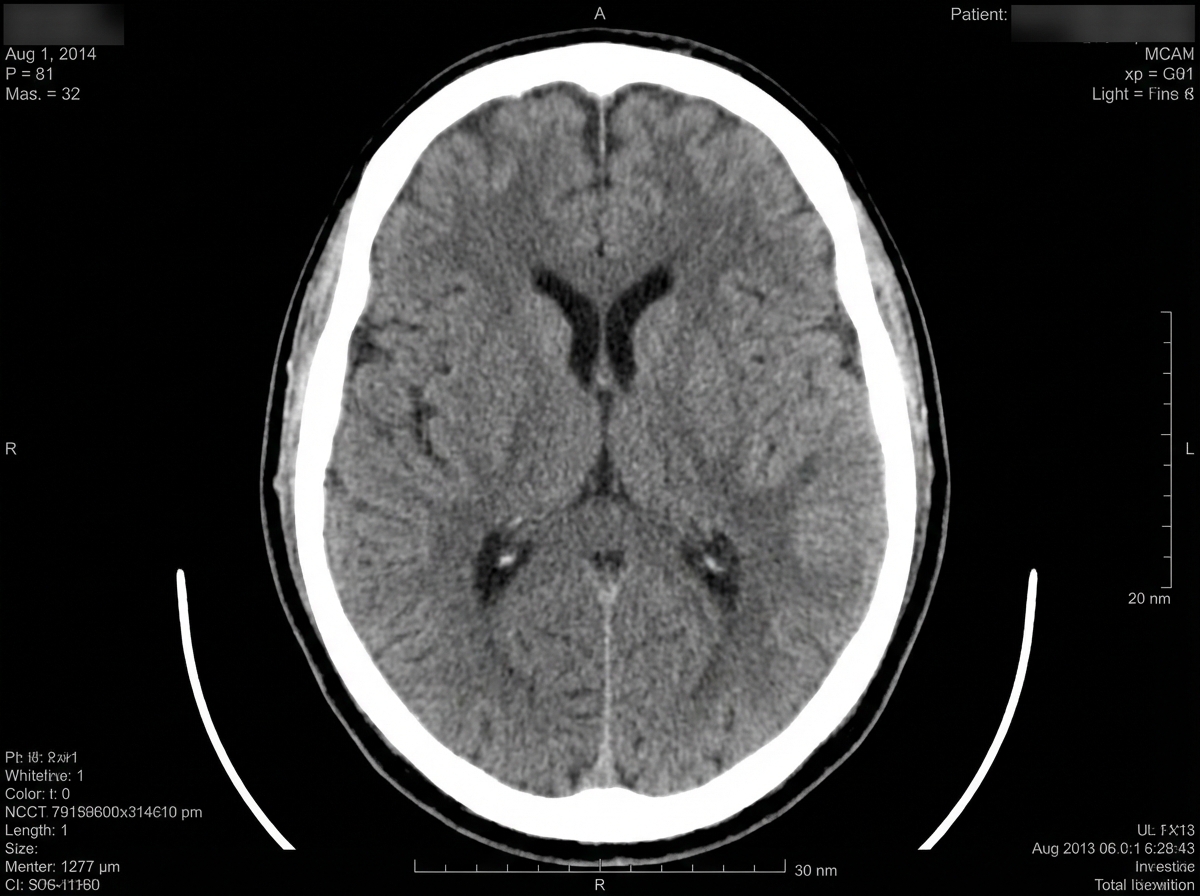
A 74-year-old right-handed woman was referred to the hospital due to concerns of a stroke. In the emergency department, the initial vital signs included blood pressure of 159/98 mm Hg, heart rate of 88/min, and respiratory rate of 20/min. She exhibited paucity of speech and apathy to her condition, although she complied with her physical examination. The initial neurologic evaluation included the following results: Awake, alert, and oriented to person, place, and time No visual field deficits Right-sided gaze deviation with full range of motion with doll’s head maneuver No facial asymmetry Grossly intact hearing No tongue deviation, equal palatal elevation, and good guttural sound production Absent pronator or lower extremity drift Decreased sensation to light touch on the right leg Normal appreciation of light touch, pressure, and pain Normal proprioception and kinesthesia Manual muscle testing: 5+ right and left upper extremities 5+ right hip, thigh, leg, and foot 3+ left hip and thigh 2+ left leg and foot A head computed tomography (CT) scan and a head magnetic resonance imaging (MRI) confirmed areas of ischemia. Which artery is the most likely site of occlusion?
A 34-year-old woman presents with fatigue, depressed mood, weight gain, and constipation. She gradually developed these symptoms over the past 6 months. She is G2P2 with the last pregnancy 9 months ago. She had a complicated delivery with significant blood loss requiring blood transfusions. She used to have a regular 28-day cycle but notes that recently it became irregular with duration lasting up to 40 days, more pain, and greater blood loss. She does not report any chronic conditions, and she is not on any medications. She is a current smoker with a 10-pack-year history. Her blood pressure is 130/80 mm Hg, heart rate is 54/min, respiratory rate is 11/min, and temperature is 35.8°C (96.4°F). Her skin is dry and pale with a fine scaling over the forearms and shins. There is a mild, non-pitting edema of the lower legs. Her lungs are clear to auscultation. Cardiac auscultation does not reveal any pathological sounds or murmurs although S1 and S2 are dulled at all points of auscultation. The abdomen is mildly distended and nontender on palpation. Neurological examination is significant for decreased deep tendon reflexes. Her blood tests show the following results: Erythrocytes count 3.4 million/mm3 Hb 12.2 mg/dL MCV 90 μm3 Reticulocyte count 0.3% Leukocyte count 5,600/mm3 Serum vitamin B12 210 ng/mL T4 total 1.01 μg/dL T4 free 0.6 ng/dL TSH 0.2 μIU/mL Which of the following lab values should be used to monitor treatment in this patient?
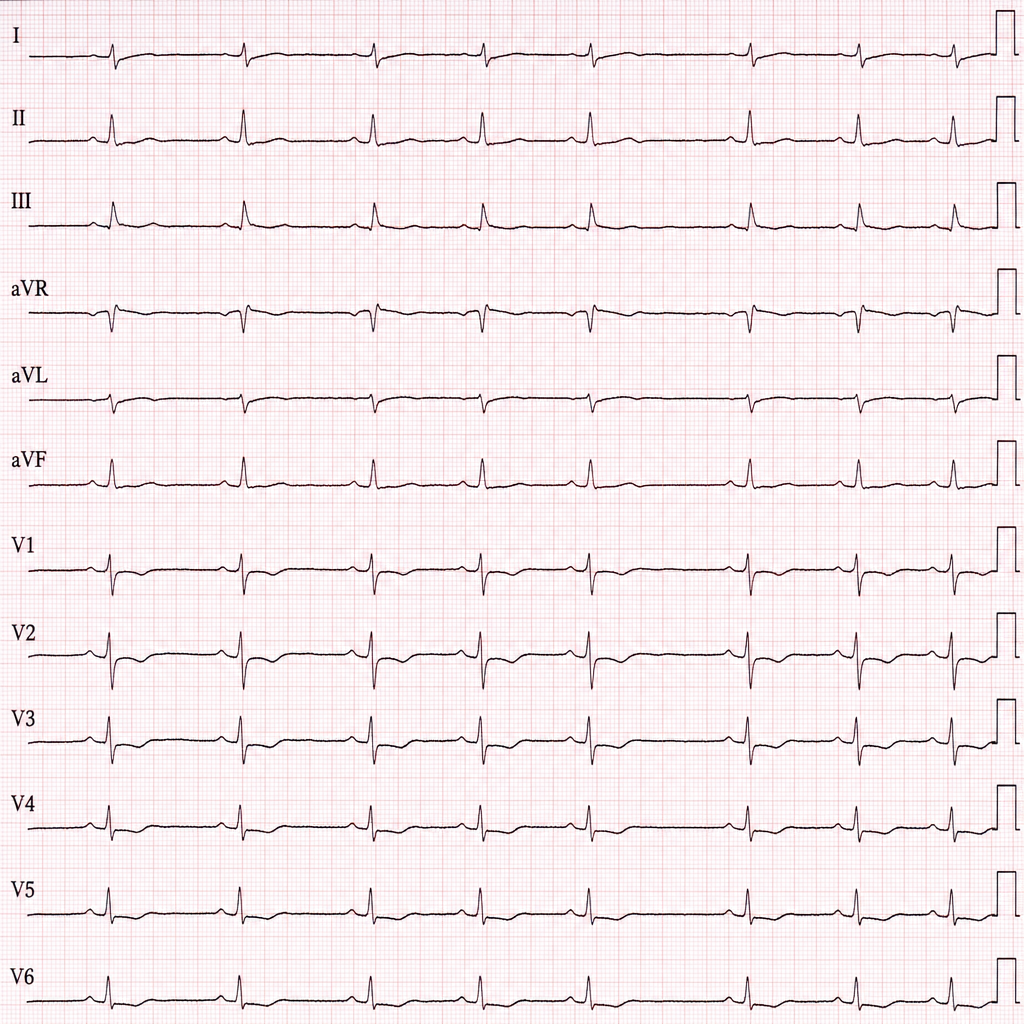
A 54-year-old man comes to the emergency department because of worsening shortness of breath, bilateral leg swelling, and constant chest pain which is not related to exertion for the last 2 weeks. The patient underwent an aortic valve replacement surgery for chronic aortic regurgitation 1 year ago, and his postoperative course was uncomplicated. He denies smoking or alcohol use. His blood pressure is 80/50 mm Hg, temperature is 36.6°C (97.9°F), and pulse is regular at 110/min. On physical examination, jugular veins are distended, +1 pitting edema is present on both ankles, and heart sounds are distant. Transthoracic echocardiography shows large pericardial effusion, chamber collapse, and respiratory variation of ventricular filling. ECG is shown in the exhibit. Which of the following findings will most likely be seen on this patient's ECG?
A 38-year-old woman presents with worsening fatigue and difficulty talking for the last few hours. Past medical history is significant for type 2 diabetes mellitus, managed with metformin and insulin. Additional current medications are a pill to ''calm her nerves'' that she takes when she has to perform live on stage for work. On physical examination, the patient is lethargic, easily confused, and has difficulty responding to questions or commands. There is also significant diaphoresis of the face and trunk present. Which of the following is the most likely etiology of this patient’s current symptoms?
A 67-year-old woman comes to the clinic complaining of progressive fatigue over the past 4 months. She noticed that she is feeling increasingly short of breath after walking the same distance from the bus stop to her home. She denies chest pain, syncope, lower extremity edema, or a cough. She denies difficulty breathing while sitting comfortably, but she has increased dyspnea upon walking or other mildly strenuous activity. Her past medical history includes mild osteoporosis and occasional gastric reflux disease. She takes oral omeprazole as needed and a daily baby aspirin. The patient is a retired accountant and denies smoking history, but she does admit to 1 small glass of red wine daily for the past 5 years. Her diet consists of a Mediterranean diet that includes fruits, vegetables, and fish. She states that she has been very healthy previously, and managed her own health without a physician for the past 20 years. On physical examination, she has a blood pressure of 128/72 mm Hg, a pulse of 87/min, and an oxygen saturation of 94% on room air. HEENT examination demonstrates mild conjunctival pallor. Lung and abdominal examinations are within normal limits. Heart examination reveals a 2/6 systolic murmur at the right upper sternal border. The following laboratory values are obtained: Hematocrit 29% Hemoglobin 9.8 g/dL Mean red blood cell volume 78 fL Platelets 240,000/mm3 White blood cells 6,000/mm3 What is the most likely reticulocyte range for this patient?
A 20-year-old female with type I diabetes mellitus presents to the emergency department with altered mental status. Her friend said that she has been out late either studying for upcoming tests or attending prayer group meetings. As far as the friend can recollect, the patient appeared to be in her usual state of health until only two days ago, when she was prescribed trimethoprim-sulfamethoxazole for a urinary tract infection. The patient complained that the medication was making her feel nauseous and bloated. The patient also relies on glargine and lispro for glycemic control. Her temperature is 100.5°F (38.1°C), blood pressure is 95/55 mmHg, pulse is 130/min, and respirations are 30/min. Her pupils are equal and reactive to light bilaterally. The remainder of the physical exam is unremarkable. Her basic metabolic panel is displayed below: Serum: Na+: 116 mEq/L Cl-: 90 mEq/L K+: 5.0 mEq/L HCO3-: 2 mEq/L BUN: 50 mg/dL Glucose: 1,200 mg/dL Creatinine: 1.5 mg/dL Which of the following is true regarding this patient's presentation?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app