
Cardiology — MCQs

On this page
Which of the following flow recording is shown below?
A hypokalemic patient develops syncope with hypotension in ICU. Name the ECG abnormality with preferred drug to be used. (Recent NEET Pattern 2016-17)
The ECG shows presence of ST elevation from V2-V5. What is the diagnosis?
In a patient with the ECG shown below, which drug is not to be given?
Identify the condition shown in the ECG given below.
Cardiology US Medical PG Practice Questions and MCQs
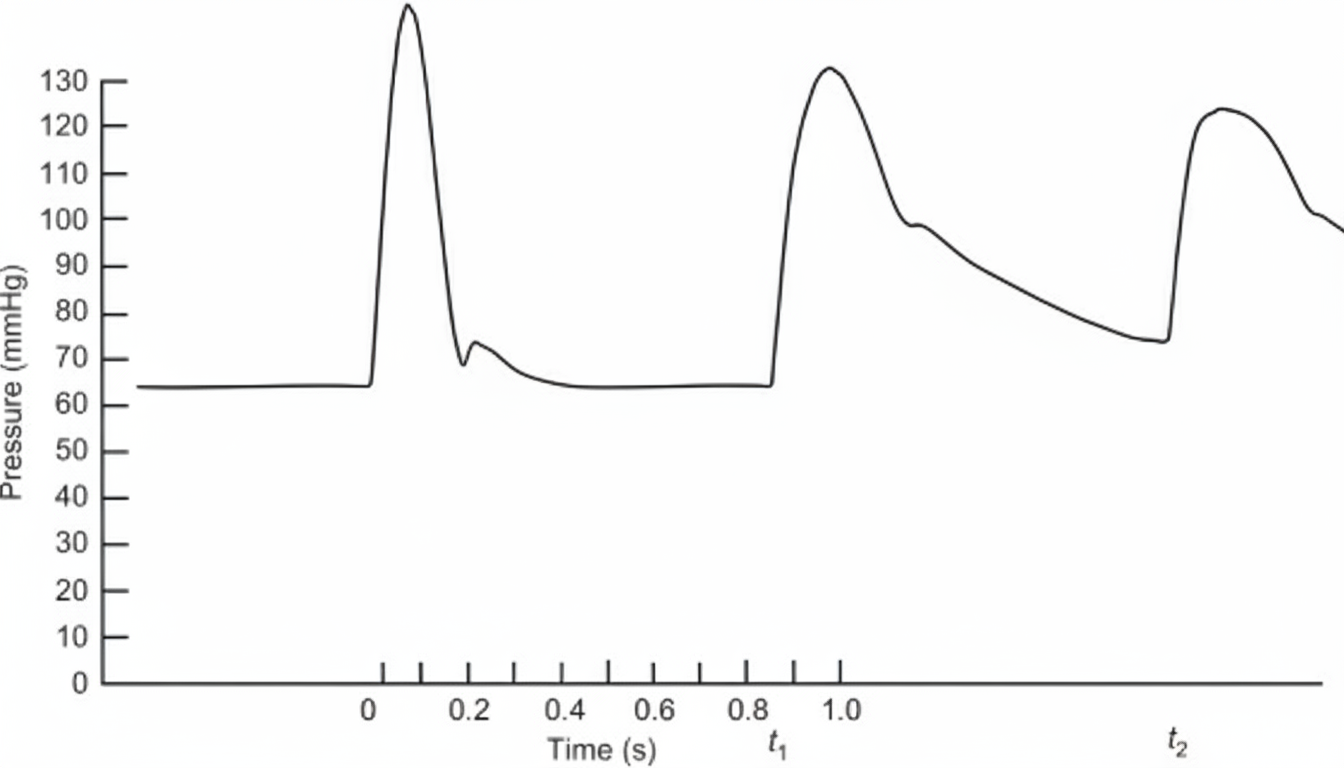
Question 1: Which of the following flow recording is shown below?
- A. Aorta flow recording (Correct Answer)
- B. Left ventricular flow recording
- C. Swan Ganz catheter tracing
- D. Coronary blood flow
- E. Pulmonary artery flow recording
Explanation: ***Aorta flow recording*** - This tracing depicts the typical **phasic flow in the aorta**, with a rapid increase during **systole** as blood is ejected from the left ventricle, followed by a decrease during **diastole**. - The graph clearly labels "Systole" and "Diastole," and the y-axis shows pressure in **mm/Hg**, which is characteristic of arterial pressure recordings. *Left ventricular flow recording* - Left ventricular (LV) pressure recordings typically show a rapid rise during **isovolumetric contraction**, a sustained peak during ejection, and a rapid fall during **isovolumetric relaxation**. - LV flow (or volume) recordings would specifically show changes in the amount of blood within the ventricle, which is not what this graph represents. *Swan Ganz catheter tracing* - A Swan-Ganz catheter, or pulmonary artery catheter, measures pressures in the **right atrium, right ventricle, pulmonary artery**, and **pulmonary capillary wedge pressure**. - The waveform associated with a Swan-Ganz catheter varies depending on its location and would not display the characteristic aortic pressure waveform shown. *Coronary blood flow* - **Coronary blood flow** refers to the blood supply to the heart muscle itself and typically has a pattern where flow is highest during **diastole** (due to ventricular compression of coronary arteries during systole). - The presented graph shows flow peaking during systole, which is inconsistent with coronary blood flow dynamics. *Pulmonary artery flow recording* - **Pulmonary artery flow** would show a similar systolic peak but with significantly **lower pressures** (typically 25/10 mm Hg) compared to the aorta (120/80 mm Hg). - The pressure magnitude shown in this tracing is consistent with **systemic arterial pressure**, not pulmonary arterial pressure.
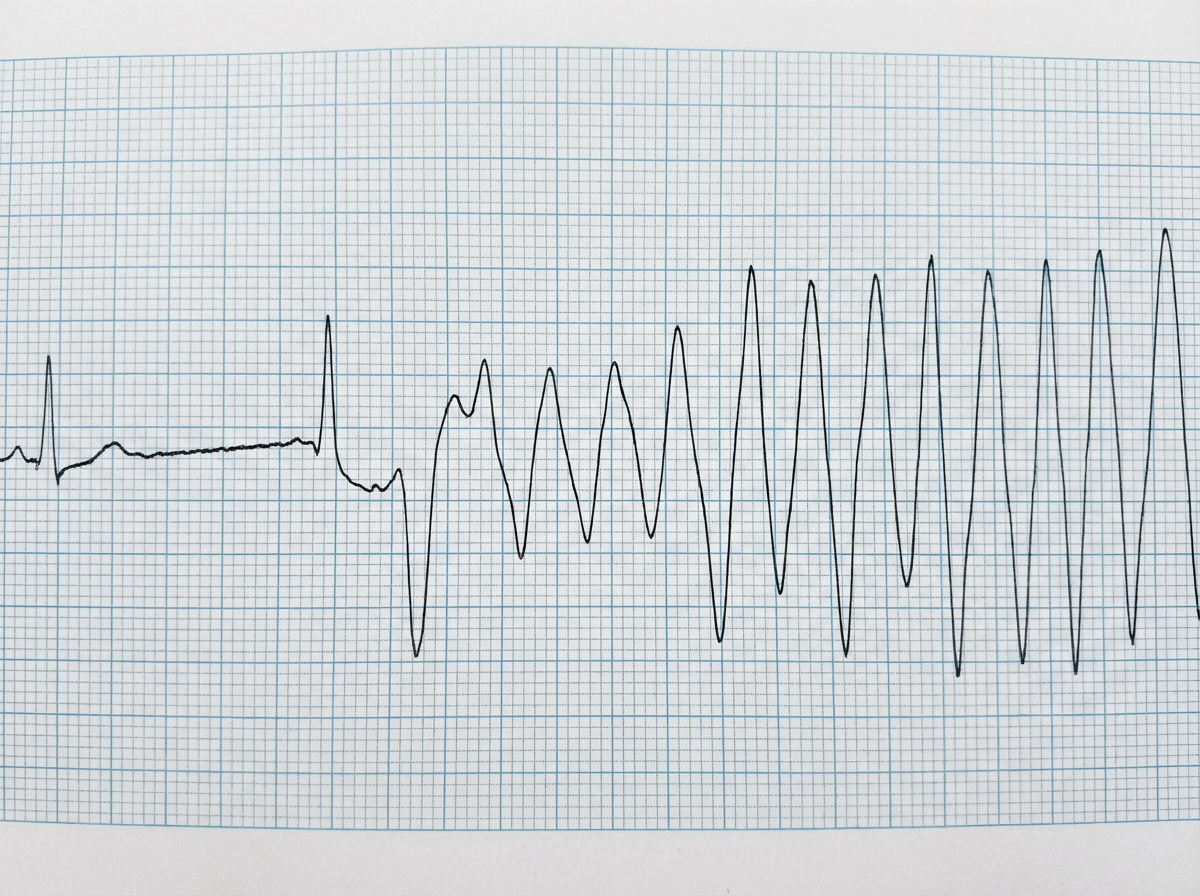
Question 2: A hypokalemic patient develops syncope with hypotension in ICU. Name the ECG abnormality with preferred drug to be used. (Recent NEET Pattern 2016-17)
- A. Ventricular fibrillation, Bretylium
- B. Ventricular tachycardia, lignocaine
- C. Torsades de pointes, Magnesium sulfate (Correct Answer)
- D. Paroxysmal ventricular tachycardia, Adenosine
- E. Atrial fibrillation, Diltiazem
Explanation: ***Torsades de pointes, Magnesium sulfate*** - The ECG shows a polymorphic ventricular tachycardia with a characteristic **twisting of the QRS complexes** around the isoelectric line, known as **Torsades de pointes**. This rhythm is often triggered by **prolonged QT interval** and is frequently associated with **hypokalemia** and other electrolyte disturbances. - **Magnesium sulfate** is the preferred drug for Torsades de pointes, particularly when associated with hypokalemia or hypomagnesemia, as it stabilizes cardiac cell membranes and reduces excitability. *Ventricular fibrillation, Bretylium* - **Ventricular fibrillation (VF)** is characterized by chaotic, irregular electrical activity with no recognizable QRS complexes, leading to no effective cardiac output. The ECG here shows distinct QRS complexes, albeit abnormal and polymorphic. - While Bretylium was historically used for VF, its use has largely been superseded by other antiarrhythmic drugs like amiodarone. The ECG pattern observed is not typical of VF. *Ventricular tachycardia, lignocaine* - The ECG shows a form of ventricular tachycardia, but more specifically, it is a polymorphic type known as Torsades de pointes, not a monomorphic ventricular tachycardia. - **Lidocaine** is an antiarrhythmic often used for stable monomorphic ventricular tachycardia; however, it is less effective and potentially proarrhythmic in Torsades de pointes. *Paroxysmal ventricular tachycardia, Adenosine* - **Paroxysmal ventricular tachycardia (PVT)** refers to VT that starts and stops suddenly. While the image shows VT, the specific morphology (polymorphic, twisting QRS) points away from standard PVT. - **Adenosine** is primarily used for **supraventricular tachycardias** (SVTs) by blocking the AV node and is **contraindicated** in ventricular tachycardias as it can worsen conditions like Torsades de pointes. *Atrial fibrillation, Diltiazem* - **Atrial fibrillation** presents with irregularly irregular rhythm with absent P waves and varying RR intervals. The ECG here shows a **ventricular arrhythmia** with wide QRS complexes and characteristic twisting morphology, not atrial fibrillation. - **Diltiazem** is a calcium channel blocker used for rate control in atrial arrhythmias and is **inappropriate for ventricular tachycardia**, especially in a hemodynamically unstable patient with syncope and hypotension.
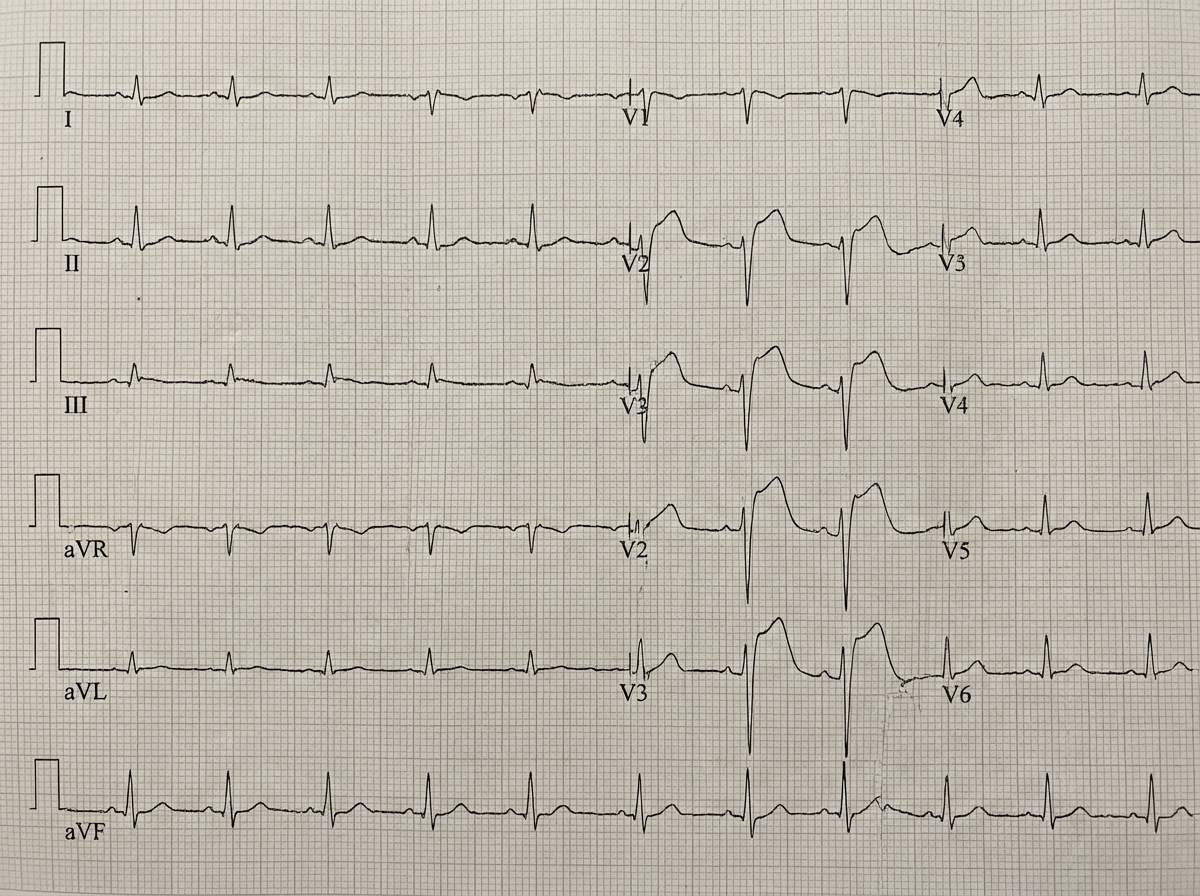
Question 3: The ECG shows presence of ST elevation from V2-V5. What is the diagnosis?
- A. Inferior wall MI
- B. Lateral wall MI
- C. Anterior wall MI (Correct Answer)
- D. Posterior wall MI
- E. Anteroseptal MI
Explanation: ***Anterior wall MI*** - **ST elevation** in leads **V2-V5** is indicative of an anterior myocardial infarction, as these leads primarily reflect the electrical activity of the anterior wall of the left ventricle. - The **anterior wall** is supplied by the **left anterior descending artery (LAD)**, and occlusion of this vessel typically results in these ECG changes. - The contiguous lead pattern from V2-V5 confirms extensive anterior wall involvement. *Inferior wall MI* - **Inferior wall MIs** are characterized by **ST elevation** in leads **II, III, and aVF**. - These leads are not primarily affected with ST elevation in the given scenario (V2-V5). *Lateral wall MI* - **Lateral wall MIs** typically show **ST elevation** in leads **I, aVL, V5, and V6**. While V5 is included, the primary elevation pattern across V2-V5 points more broadly to an anterior infarction. - Absence of ST elevation in I and aVL makes isolated lateral MI less likely. *Posterior wall MI* - A **posterior wall MI** is diagnosed by **ST depression** in leads **V1-V3** (reciprocal changes) and tall R waves in V1-V2, not ST elevation. - To confirm, posterior leads (V7-V9) would show ST elevation. *Anteroseptal MI* - **Anteroseptal MI** typically shows **ST elevation** in leads **V1-V4**, focusing on the septal region. - While there is overlap with V2-V4, the extension to V5 indicates more extensive anterior wall involvement rather than isolated anteroseptal territory.
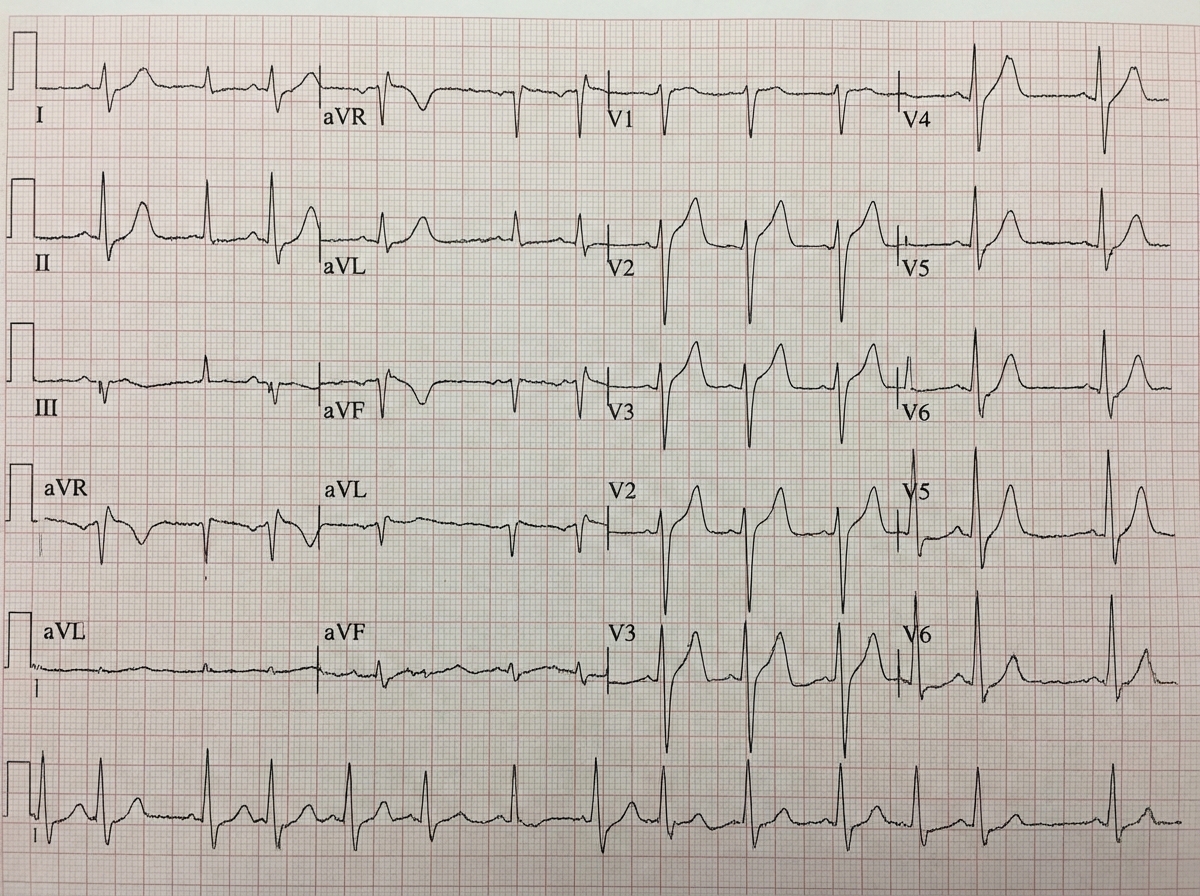
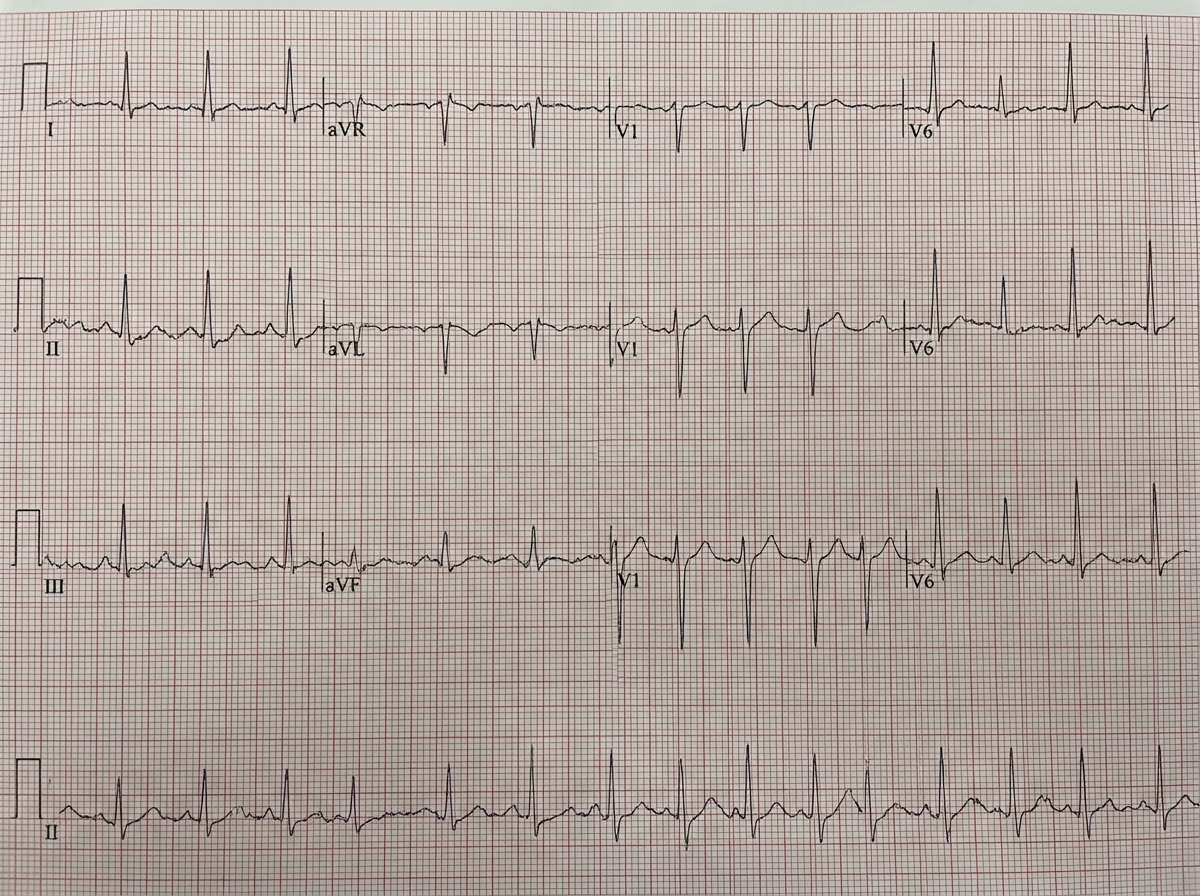
Question 4: In a patient with the ECG shown below, which drug is not to be given?
- A. Amiodarone
- B. Adenosine (Correct Answer)
- C. Diltiazem
- D. Beta blocker
- E. Procainamide
Explanation: ***Adenosine*** - The ECG shows a **wide complex tachycardia** with signs of **ventricular preexcitation** (e.g., short PR interval, delta waves in some leads like V4-6). This rhythm could represent **atrial fibrillation with Wolff-Parkinson-White (WPW) syndrome**. - **Adenosine** is **contraindicated** in patients with **WPW with atrial fibrillation** because it can block the AV node, forcing impulses down the accessory pathway, which can accelerate the heart rate and lead to **ventricular fibrillation**. - Among AV nodal blockers, adenosine poses the **most acute risk** of precipitating life-threatening arrhythmias. *Amiodarone* - **Amiodarone** is an **antiarrhythmic drug** that can be used in patients with **wide complex tachycardia**, including those with preexcitation. - It is generally considered a safer option for rate control in **AF with WPW** compared to AV nodal blocking agents. *Diltiazem* - **Diltiazem** is a **calcium channel blocker** that primarily works by **blocking the AV node**. - Similar to adenosine, **AV nodal blockers** are contraindicated in AF with WPW as they can increase conduction down the accessory pathway, posing a risk of **ventricular fibrillation**. - However, adenosine is considered the **most acutely dangerous** among AV nodal blockers. *Beta blocker* - **Beta-blockers** are also **AV nodal blocking agents** that slow conduction through the AV node. - Like adenosine and diltiazem, they are contraindicated in **AF with WPW** due to the risk of shunting impulses down the accessory pathway and potentially leading to **ventricular fibrillation**. *Procainamide* - **Procainamide** is a **class IA antiarrhythmic** that blocks both the AV node and the accessory pathway. - It is considered **first-line therapy** for hemodynamically stable **AF with WPW** as it slows conduction through the accessory pathway without the risk of accelerating ventricular rate. - It is a **safe option** in this clinical scenario.
Question 5: Identify the condition shown in the ECG given below.
- A. Sinus rhythm
- B. PSVT
- C. Atrial fibrillation (Correct Answer)
- D. Ventricular fibrillation
- E. Atrial flutter
Explanation: ***Atrial fibrillation*** - The ECG shows a rhythm that is **irregularly irregular**, which is a classic hallmark of atrial fibrillation due to chaotic atrial activity. - There is an **absence of distinct P waves**, which are replaced by fibrillatory waves (f waves) that are often subtle and variable in morphology. *Sinus rhythm* - Sinus rhythm is characterized by a **regular rhythm** originating from the sinoatrial node, with a distinct P wave before every QRS complex. - The ECG in the image clearly demonstrates an **irregular rhythm** and no clear P waves. *PSVT* - Paroxysmal supraventricular tachycardia (PSVT) typically presents with a **regular, fast heart rate** and narrow QRS complexes, with P waves often hidden within the QRS or T waves. - The rhythm in the ECG is **irregular**, not regular, ruling out typical PSVT. *Atrial flutter* - Atrial flutter is characterized by **organized atrial activity** with a regular atrial rate (typically 250-350 bpm) producing classic **"sawtooth" flutter waves** (F waves), most visible in leads II, III, and aVF. - The ventricular response may be regular or irregular depending on AV conduction, but the ECG shows **absence of organized flutter waves** and instead demonstrates chaotic fibrillatory activity. *Ventricular fibrillation* - Ventricular fibrillation (VF) is a chaotic, life-threatening arrhythmia characterized by **no discernible P waves or QRS complexes**, and a completely irregular, undulating baseline. - While the rhythm is irregular, the presence of **identifiable QRS complexes** rules out ventricular fibrillation, which involves complete disorganization of ventricular electrical activity.
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free