
Cardiology — MCQs

On this page
A 32-year-old man comes to the emergency department because of worsening shortness of breath and a productive cough for 3 days. He sustained trauma to the right hemithorax during a fight 3 weeks ago. He had significant pain and mild shortness of breath following the incident but did not seek medical care. He does not smoke or drink alcohol. He is a construction worker. His temperature is 38.4°C (101.1°F), pulse is 95/min, respirations are 18/min, and blood pressure is 120/75 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Pulmonary examination shows decreased breath sounds over the right lower lung fields. CT scan of the chest shows fractures of the right 7th and 8th ribs, right pleural splitting and thickening, and a dense fluid collection in the pleural space. Which of the following is the most likely diagnosis?
A 23-year-old man comes to the emergency department for 2 days of severe headaches. The pain is most intense on his left forehead and eye. He had similar symptoms last summer. He has been taking indomethacin every 6 hours for the last 24 hours but has not had any relief. He has smoked 1 pack of cigarettes daily for the past 5 years. He works as an accountant and describes his work as very stressful. Physical examination shows drooping of the left eyelid, tearing of the left eye, and rhinorrhea. The left pupil is 2 mm and the right pupil is 4 mm. There is localized tenderness along the right supraspinatus muscle. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 22-year-old patient presents to the rural medicine clinic for a physical examination. She has a past medical history of major depressive disorder. The patient has a history of smoking 1 pack of cigarettes daily for 5 years. She states that she is not currently sexually active, but had sexual intercourse in the past. Her paternal grandfather died of a heart attack at the age of 60. She takes citalopram by mouth once every morning. The blood pressure is 110/70 mm Hg, the heart rate is 76/min, and the respiratory rate is 12/min. Her physical examination reveals a well-nourished, alert, and oriented female. While auscultating the heart, a 2/6 holosystolic murmur at the left upper sternal border is present. Which of the following would be the most appropriate next step for this patient?
An x-ray of the chest shows an extensive consolidation within the right lower lobe consistent with lobar pneumonia. Sputum and blood cultures are sent to the laboratory for analysis, and empiric antibiotic treatment with intravenous cefotaxime is begun. Which of the following is most likely to have prevented this patient's pneumonia?
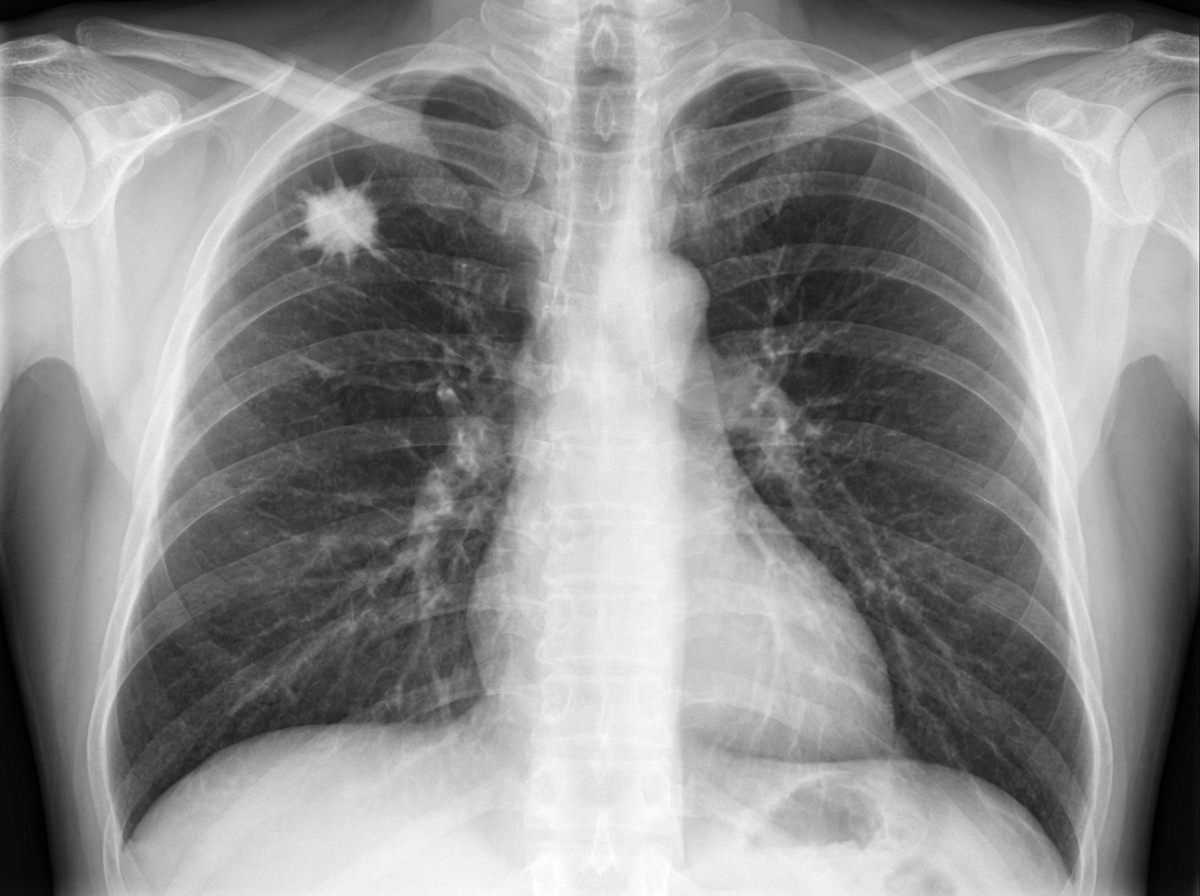
A 62-year-old man comes to the physician because of a persistent cough for the past 2 weeks. During this time, he has also had occasional discomfort in his chest. Three weeks ago, he had a sore throat, headache, and a low-grade fever, which were treated with acetaminophen and rest. He has a history of hypertension and hyperlipidemia. His father died of myocardial infarction at the age of 57 years. He has smoked a pack of cigarettes daily for the past 40 years. Current medications include enalapril and atorvastatin. His temperature is 37°C (98.6°F), pulse is 70/min, and blood pressure is 145/90 mm Hg. Physical examination shows no abnormalities. An x-ray of the chest is shown. Which of the following is the most appropriate next step in management?
A 35-year-old man comes to the physician because of a rash on the thigh for 10 days. He reports that the rash has been enlarging and is intensely itchy. Two weeks ago, he adopted a stray dog from an animal shelter. Vital signs are within normal limits. A photograph of the examination findings is shown. Which of the following is the most likely cause of this patient's symptoms?

A 74-year-old African-American woman is brought to the emergency department by her home health aid. The patient was eating breakfast this morning when she suddenly was unable to lift her spoon with her right hand. She attempted to get up from the table, but her right leg felt weak. One hour later in the emergency department, her strength is 0/5 in the right upper and right lower extremities. Strength is normal in her left upper and lower extremities. Sensation is normal bilaterally. An emergency CT of the head does not show signs of hemorrhage. Subsequent brain MRI shows an infarct involving the internal capsule. Which of the following is true about her disease process?
A 68-year-old man is admitted to the intensive care unit after open abdominal aortic aneurysm repair. The patient has received 4 units of packed red blood cells during the surgery. During the first 24 hours following the procedure, he has only passed 200 mL of urine. He has congestive heart failure and hypertension. Current medications include atenolol, enalapril, and spironolactone. He appears ill. His temperature is 37.1°C (98.8°F), pulse is 110/min, respirations are 18/min, and blood pressure is 110/78 mm Hg. Examination shows dry mucous membranes and flat neck veins. The remainder of the examination shows no abnormalities. Laboratory studies show a serum creatinine level of 2.0 mg/dL and a BUN of 48 mg/dL. His serum creatinine and BUN on admission were 1.2 mg/dL and 18 mg/dL, respectively. Further evaluation of this patient is most likely to reveal which of the following findings?
A 15-year-old girl is hospitalized because of increased fatigue and weight loss over the past 2 months. The patient has no personal or family history of a serious illness. She takes no medications, currently. Her blood pressure is 175/74 mm Hg on the left arm and 90/45 on the right. The radial pulse is 84/min but weaker on the right side. The femoral blood pressure and pulses show no abnormalities. Temperature is 38.1℃ (100.6℉). The muscles over the right upper arm are slightly atrophic. The remainder of the examination reveals no abnormalities. Laboratory studies show the following results: Hemoglobin 10.4 g/dL Leukocyte count 5,000/mm3 Erythrocyte sedimentation rate 58 mm/h Magnetic resonance arteriography reveals irregularity, stenosis, and poststenotic dilation involving the proximal right subclavian artery. Prednisone is initiated with improvement of her symptoms. Which of the following is the most appropriate next step in the patient management?
A 37-year-old woman accompanied by her husband presents to the emergency department after loss of consciousness 30 minutes ago. The husband reports that she was sitting in a chair at home and began having sustained rhythmic contractions of all 4 extremities for approximately 1 minute. During transport via ambulance she appeared confused but arousable. Her husband reports she has no medical conditions, but for the past 2 months she has occasionally complained of episodes of sweating, palpitations, and anxiety. Her brother has epilepsy and her mother has type 1 diabetes mellitus. Laboratory studies obtained in the emergency department demonstrate the following: Serum: Na+: 136 mEq/L K+: 3.8 mEq/L Cl-: 100 mEq/L HCO3-: 19 mEq/L BUN: 16 mg/dL Creatinine: 0.9 mg/dL Glucose: 54 mg/dL C-peptide: Low Which of the following is the most likely diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app