
Cardiology — MCQs

On this page
A patient presents with cold skin, fatigue, shortness of breath on exertion, and an enlarged liver. Upon examination, his jugular venous pressure (JVP) reveals a prominent "a" wave. What is the most likely cause of the elevated "a" wave in this patient?
A 45-year-old male with a 15-year history of diabetes mellitus presents to his primary care provider for a routine checkup. His doctor is concerned about his renal function and would like to order a test to detect renal impairment. Which of the following is the most sensitive test for detecting renal impairment in diabetic patients?
A 61-year-old man presents to his primary care provider with fatigue, weight loss, and muscle aches. He has experienced these symptoms for the past year but initially attributed them to stress at his work as an attorney. However, over the past month, he has developed intermittent fevers associated with a skin rash that prompted him to seek medical evaluation. He denies any recent history of asthma, rhinitis, hematuria, or difficulty breathing. He is otherwise healthy and takes no medications. He has a distant history of cocaine abuse but has not used any drugs in 30 years. His family history is notable for pancreatic cancer in his father and inflammatory bowel disease in his sister. His temperature is 99.3°F (37.4°C), blood pressure is 130/75 mmHg, pulse is 90/min, and respirations are 18/min. On examination, rales are heard at the bilateral lung bases. S1 and S2 are normal. Strength is 5/5 in the bilateral upper and lower extremities and his gait is normal. Palpable purpura are noted on his trunk and bilateral upper and lower extremities. Erythrocyte sedimentation rate and C-reactive protein are both elevated. This patient’s condition is associated with antibodies directed against which of the following enzymes?
A 25-year-old man presents to his physician for new-onset palpitations and tremors in his right hand. He also feels more active than usual, but with that, he is increasingly feeling fatigued. He lost about 3 kg (6.6 lb) in the last 2 months and feels very anxious about his symptoms. He survived neuroblastoma 15 years ago and is aware of the potential complications. On examination, a nodule around the size of 2 cm is palpated in the right thyroid lobule; the gland is firm and nontender. There is no lymphadenopathy. His blood pressure is 118/75 mm Hg, respirations are 17/min, pulse is 87/min, and temperature is 37.5°C (99.5°F). Which of the following is the best next step in the management of this patient?
A 28-year-old man presents to the emergency department after being rescued from his home. He was working at home alone on some renovations when 1 of his house's walls collapsed on him. His legs were trapped under the debris for about 30 hours before a neighbor came by, found him, and called an ambulance. He is very mildly confused and reports pain throughout both legs. The physical examination is notable for dry mucous membranes and tenderness to palpation throughout both legs with many superficial abrasions, but no active hemorrhage. The full-body computed tomography (CT) scan shows small fractures in both tibias, but no hematomas. He is admitted to the trauma service for observation. On hospital day 1, his urine appears very dark. Urine output over the preceding 24 hours is 200 mL. The laboratory studies show a creatinine of 2.7 mg/dL and serum creatine kinase (CK) of 29,700 IU/L. Which of the following is the next best step in the management of this patient?
A 42-year-old woman comes to the physician because of frequent episodes of headaches and tinnitus over the past 3 months. One week ago, she had a brief episode of left arm weakness and numbness that lasted for 2 minutes before spontaneously resolving. She is otherwise healthy and takes no medications. She has smoked one-half pack of cigarettes daily for 22 years. Her pulse is 84/min and blood pressure is 155/105 mm Hg. Abdominal examination shows no masses or tenderness. A bruit is heard on auscultation of the abdomen. Abdominal ultrasonography shows a small right kidney. CT angiography shows stenosis of the distal right renal artery. Which of the following is the most likely underlying cause of the patient's condition?
A 55-year-old Caucasian woman visits her family physician for a checkup and to discuss her laboratory results from a previous visit. The medical history is significant for obesity, hypothyroidism, and chronic venous insufficiency. The medications include thyroxine and a multivitamin. In her previous visit, she complained about being hungry all the time, urinating multiple times a day, and craving water for most of the day. Blood and urine samples were obtained. Today her blood pressure is 120/70 mm Hg, the pulse is 80/min, the respiratory rate is 18/min, and the body temperature is 36.4°C (97.5°F). The physical examination reveals clear lungs with regular heart sounds and no abdominal tenderness. There is mild pitting edema of the bilateral lower extremities. The laboratory results are as follows: Elevated SCr for an eGFR of 60 mL/min/1.73 m² Spot urine albumin-to-creatinine ratio 250 mg/g Urinalysis Specific gravity 1.070 Proteins (++) Glucose (+++) Nitrites (-) Microscopy Red blood cells none White blood cells none Hyaline casts few A bedside renal ultrasound revealed enlarged kidneys bilaterally without hydronephrosis. Which of the following kidney-related test should be ordered next?
A 44-year-old woman presents to her primary care physician’s office with episodes of pain in her right hand. She says that the pain is most significant at night and awakens her from sleep numerous times. When she experiences this pain, she immediately puts her hand under warm running water or shakes her hand. She has also experienced episodes of numbness in the affected hand. Driving and extending the right arm also provoke her symptoms. She denies any trauma to the hand or associated weakness. Medical history is notable for hypothyroidism treated with levothyroxine. She works as a secretary for a law firm. On physical exam, when the patient hyperflexes her wrist, pain and paresthesia affect the first 3 digits of the right hand. Which of the following is the confirmatory diagnostic test for this patient?
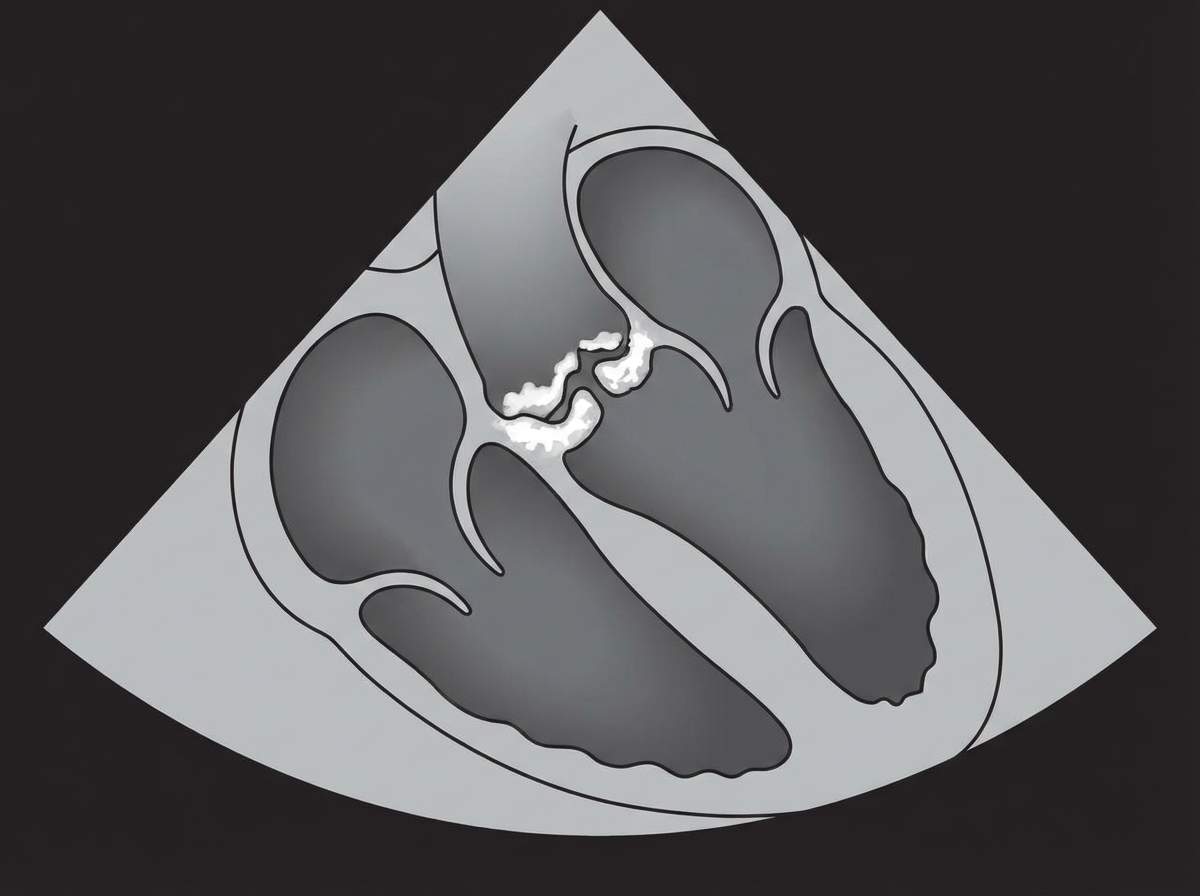
An 81-year-old man comes to the physician because of increased exertional dyspnea and dizziness over the past 8 weeks. He has hypertension for which he takes lisinopril. He has smoked one pack of cigarettes daily for the past 50 years. Physical examination shows weak peripheral pulses. Cardiac examination is shown. Which of the following is the most likely diagnosis?
A 31-year-old woman presents to the physician for a routine health maintenance examination. She feels well and has no current complaints. She has no history of serious illness and takes no medications. The vital signs include: blood pressure 185/110 mm Hg, pulse 75/min, and respiration rate 12/min. Her high blood pressure is confirmed during a 2nd visit. Neurologic examination shows no abnormalities. Careful auscultation of the abdomen reveals bruits in both upper quadrants near the midline. The remainder of the physical exam is unremarkable. The results of a complete blood count (CBC), renal function panel, and urinalysis showed no abnormalities. Conventional angiography confirms bilateral disease involvement. To control this patient’s hypertension, it is most appropriate to recommend which of the following?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app