
Cardiology — MCQs

On this page
A 55-year-old man presents to the physician with tiredness, lethargy, bone pain, and colicky right abdominal pain for 1 month. He has no comorbidities. He does not have any significant past medical history. His height is 176 cm (5 ft 7 in), weight is 88 kg (194 lb), and his BMI is 28.47 kg/m2. The physical examination is normal, except for mild right lumbar region tenderness. Laboratory studies show: Hemoglobin 13.5 g/dL Serum TSH 2.2 mU/L Serum calcium 12.3 mg/dL Serum phosphorus 1.1 mg/dL Serum sodium 136 mEq/L Serum potassium 3.5 mEq/L Serum creatinine 1.1 mg/dL Urine calcium Elevated An ultrasound of the abdomen reveals a single stone in the right ureter without hydroureteronephrosis. Clinically, no evidence of malignancy was observed. An X-ray of the long bones reveals diffuse osteopenia with subperiosteal bone resorption. The serum parathyroid hormone level is tested and it is grossly elevated. What is the most appropriate next step in his management?
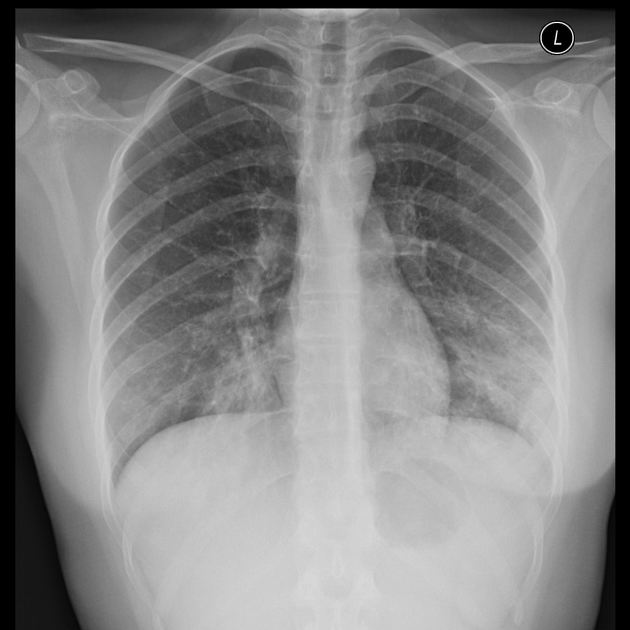
A 24-year-old woman, otherwise healthy, presents with a non-productive cough, sore throat, and myalgia. The patient reports that her symptoms started gradually 2 weeks ago and have not improved. She has no significant past medical history and no current medications. She is a college student and denies any recent overseas travel. The patient received the flu vaccine this year, and her 2-part PPD required for school was negative. She does not smoke, drink, or use recreational drugs. The patient denies being sexually active. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 110/75 mm Hg, pulse 98/min, respirations 20/min, and oxygen saturation 99% on room air. On physical exam, the patient is alert and cooperative. The cardiac exam is normal. There are rales present bilaterally over both lung fields. The skin and conjunctiva are pale. The laboratory tests are pending. The chest X-ray is shown in the image. Which of the following laboratory findings would also commonly be found in this patient?
A 32-year-old man comes to the emergency room because of severe breathlessness for the past few hours. Over the course of a few years, he has been treated for asthma by several physicians, but his symptoms have continued to progress. He has never smoked. Both his father who died at the age of 40 years and his uncle (father's brother), died with chronic obstructive pulmonary disorder. His respiratory rate is 19/min and temperature is 37.0°C (98.6°F). On physical examination, the patient has significantly longer exhalation than inhalation. His expiratory time is longer than 6 seconds. Clubbing is present. Chest auscultation reveals bilateral crackles. Mild hepatomegaly is present. What is the most likely diagnosis?
A 72-year-old man comes to the physician because of a 2-month history of intermittent retrosternal chest pain and tightness on exertion. He has type 2 diabetes mellitus, osteoarthritis of the right hip, and hypertension. Current medications include insulin, ibuprofen, enalapril, and hydrochlorothiazide. Vital signs are within normal limits. His troponin level is within the reference range. An ECG at rest shows a right bundle branch block and infrequent premature ventricular contractions. The patient's symptoms are reproduced during adenosine stress testing. Repeat ECG during stress testing shows new ST depression of > 1 mm in leads V2, V3, and V4. Which of the following is the most important underlying mechanism of this patient's ECG changes?
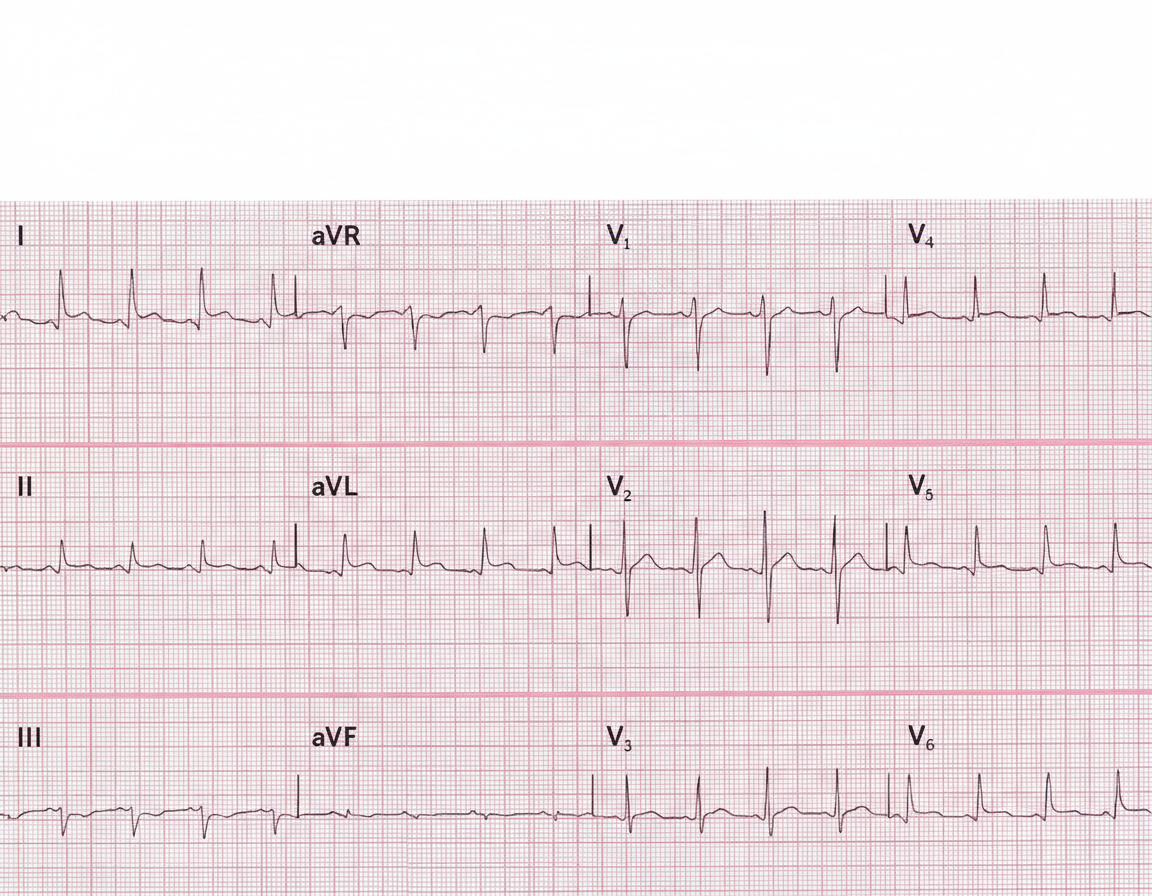
A 29-year-old man presents to the emergency department with a sharp pain in the center of his chest. The pain is knife-like and constant. Sitting alleviates the pain and lying supine aggravates it. He denies the use of nicotine, alcohol or illicit drugs. Vital signs include: temperature 37.0°C (98.6°F), blood pressure 135/92 mm Hg, and pulse 97/min. On examination, a friction rub is heard at the left sternal border while the patient is leaning forward. His ECG is shown in the image. Which of the following can prevent recurrence of this patient’s condition?
A 47-year-old woman with a long history of poorly controlled type 2 diabetes and recurrent urinary tract infections presents with complaints of fever, chills, and severe flank pain. On physical exam, she has left-sided costovertebral tenderness. Vitals include a temperature of 39.4°C (103.0°F), blood pressure of 125/84 mm Hg, and pulse of 84/min. She is currently taking metformin daily. Urine dipstick analysis is positive for leukocytes, nitrites, and blood. Laboratory studies show an elevated creatinine of 2.8 mg/dL (baseline 1.0 mg/dL). Urinalysis reveals fragments of tissue. What is the most likely diagnosis?
A 17-year-old girl comes to the physician because of a sore throat, fevers, and fatigue for the past 3 weeks. Her temperature is 37.8°C (100°F), pulse is 97/min, and blood pressure is 90/60 mm Hg. Examination of the head and neck shows cervical lymphadenopathy, pharyngeal erythema, enlarged tonsils with exudates, and palatal petechiae. The spleen is palpated 2 cm below the left costal margin. Her leukocyte count is 14,100/mm3 with 54% lymphocytes (12% atypical lymphocytes). Results of a heterophile agglutination test are positive. This patient is at increased risk for which of the following conditions?
A 50-year-old man presents to the emergency department with pain and swelling of his right leg for the past 2 days. Three days ago he collapsed on his leg after tripping on a rug. It was a hard fall and left him with bruising of his leg. Since then the pain and swelling of his leg have been gradually increasing. Past medical history is noncontributory. He lives a rather sedentary life and smokes two packs of cigarettes per day. The vital signs include heart rate 98/min, respiratory rate 15/min, temperature 37.8°C (100.1°F), and blood pressure 100/60 mm Hg. On physical examination, his right leg is visibly swollen up to the mid-calf with pitting edema and moderate erythema. Peripheral pulses in the right leg are weak and the leg is tender. Manipulation of the right leg is negative for Homan’s sign. What is the next best step in the management of this patient?
A 78-year-old man is brought to the emergency department because of difficulty speaking. The symptoms began abruptly one hour ago while he was having breakfast with his wife. He has hypertension, type 2 diabetes mellitus, and coronary artery disease. Current medications include pravastatin, lisinopril, metformin, and aspirin. His temperature is 37°C (98.6°F), pulse is 76/min, and blood pressure is 165/90 mm Hg. He is right-handed. The patient speaks in short, simple sentences, and has difficulty repeating sequences of words. He can follow simple instructions. Right facial droop is present. Muscle strength is 4/5 on the right side and 5/5 on the left, and there is a mild right-sided pronator drift. Which of the following is the most likely cause of the patient's symptoms?
A 44-year-old male presents to his primary care physician with complaints of fatigue, muscle weakness, cramps, and increased urination over the past several weeks. His past medical history is significant only for hypertension, for which he was started on hydrochlorothiazide (HCTZ) 4 weeks ago. Vital signs at today's visit are as follows: T 37.2, HR 88, BP 129/80, RR 14, and SpO2 99%. Physical examination does not reveal any abnormal findings. Serologic studies are significant for a serum potassium level of 2.1 mEq/L (normal range 3.5-5.0 mEq/L). Lab-work from his last visit showed a basic metabolic panel and complete blood count results to all be within normal limits. Which of the following underlying diseases most likely contributed to the development of this patient's presenting condition?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app