
Cardiology — MCQs

On this page
A 48-year-old woman is transferred from her primary care physician's office to the emergency department for further evaluation of hypokalemia to 2.5 mEq/L. She was recently diagnosed with hypertension 2 weeks ago and started on medical therapy. The patient said that she enjoys all kinds of food and exercises regularly, but has not been able to complete her workouts as she usually does. Her temperature is 97.7°F (36.5°C), blood pressure is 107/74 mmHg, pulse is 80/min, respirations are 15/min, and SpO2 is 94% on room air. Her physical exam is unremarkable. Peripheral intravenous (IV) access is obtained. Her basic metabolic panel is obtained below. Serum: Na+: 135 mEq/L Cl-: 89 mEq/L K+: 2.2 mEq/L HCO3-: 33 mEq/L BUN: 44 mg/dL Glucose: 147 mg/dL Creatinine: 2.3 mg/dL Magnesium: 2.0 mEq/L What is the next best step in management?
A 22-year-old woman presents to the emergency department with a chief concern of shortness of breath. She was hiking when she suddenly felt unable to breathe and had to take slow deep breaths to improve her symptoms. The patient is a Swedish foreign exchange student and does not speak any English. Her past medical history and current medications are unknown. Her temperature is 99.5°F (37.5°C), blood pressure is 127/68 mmHg, pulse is 120/min, respirations are 22/min, and oxygen saturation is 90% on room air. Physical exam is notable for poor air movement bilaterally and tachycardia. The patient is started on treatment. Which of the following best describes this patient's underlying pathology? FEV1 = Forced expiratory volume in 1 second FVC = Forced vital capacity DLCO = Diffusing capacity of carbon monoxide
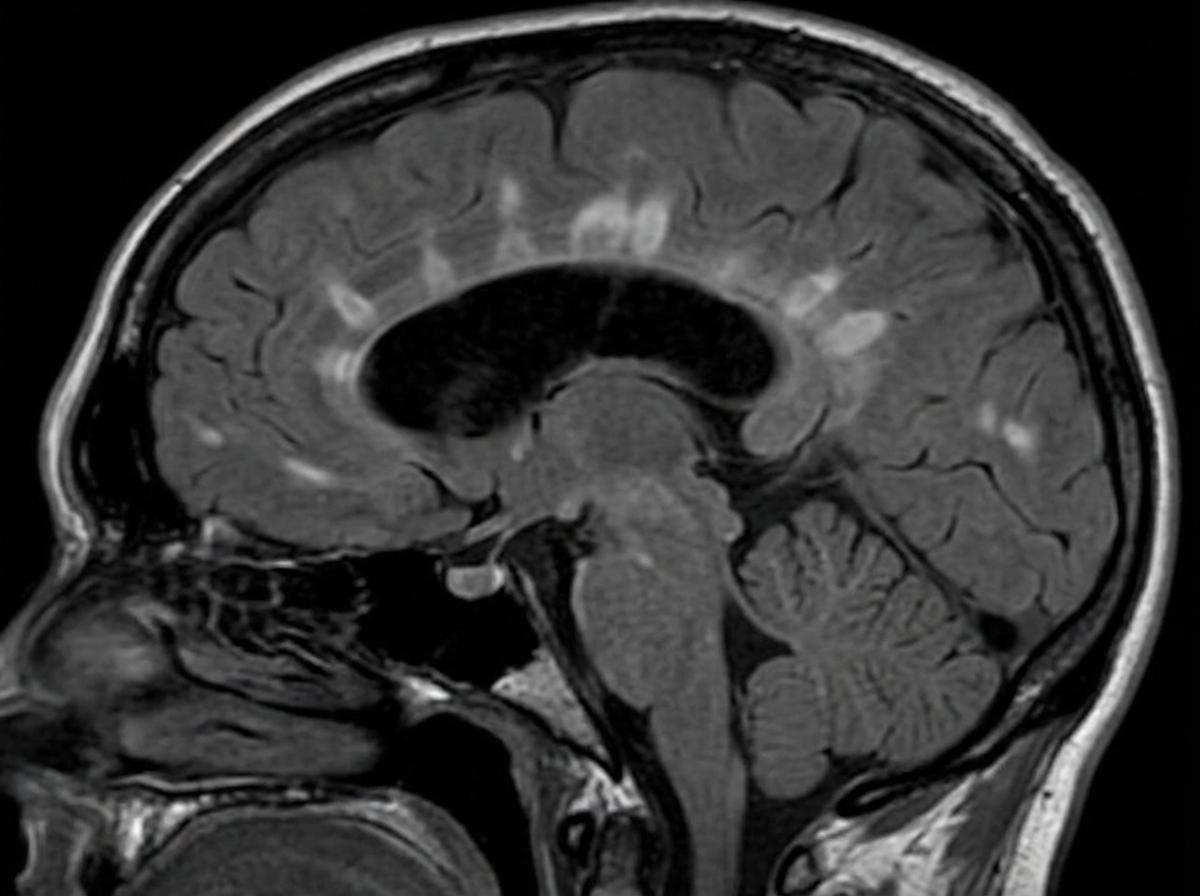
A 29-year-old woman presents with progressive vision loss in her right eye and periorbital pain for 5 days. She says that she has also noticed weakness, numbness, and tingling in her left leg. Her vital signs are within normal limits. Neurological examination shows gait imbalance, positive Babinski reflexes, bilateral spasticity, and exaggerated deep tendon reflexes in the lower extremities bilaterally. FLAIR MRI is obtained and is shown in the image. Which of the following is the most likely cause of this patient's condition?
A 34-year-old man presents with multiple painful ulcers on his penis. He says that the ulcers all appeared suddenly at the same time 3 days ago. He reports that he is sexually active with multiple partners and uses condoms inconsistently. He is afebrile and his vital signs are within normal limits. Physical examination reveals multiple small shallow ulcers with an erythematous base and without discharge. There is significant inguinal lymphadenopathy present. Which of the following is the most likely etiologic agent of this patient’s ulcers?
A 35-year-old woman presents to the clinic for a several-month history of heat intolerance. She lives in a small apartment with her husband and reports that she always feels hot and sweaty, even when their air conditioning is on high. On further questioning, she's also had a 4.5 kg (10 lb) unintentional weight loss. The vital signs include: heart rate 102/min and blood pressure 150/80 mm Hg. The physical exam is notable for warm and slightly moist skin. She also exhibits a fine tremor in her hands when her arms are outstretched. Which of the following laboratory values is most likely low in this patient?
A 64-year-old man presents with a complaint of prominent stiffness in his legs which is causing a difficulty in ambulation. He is not able to relax his trunk area and has frequent, painful muscle spasms. He denies diplopia, swallowing difficulties, and urinary or bowel problems. He has a medical history of stage IV lung cancer. He has received 4 sessions of chemotherapy. The neurological examination reveals an increased generalized muscle tone. He has a spastic gait with exaggerated lumbar lordosis. The needle electromyography (EMG) studies show continuous motor unit activity that persists at rest. Which paraneoplastic antibody is most likely associated with the symptoms of this patient?
A 55-year-old woman sees her family doctor for a follow-up appointment to discuss her imaging studies. She previously presented with chest pain and shortness of breath for the past 2 months. Her CT scan shows a 3.5 cm mass in the lower lobe of her right lung. The mass has irregular borders. Saddle/hilar lymph nodes are enlarged. No distant metastases are identified with PET imaging. The patient has been a smoker for over 35 years (1.5 packs per day), but she has recently quit. This patient is referred to the Pulmonary Diseases Center. What is the most effective step in appropriately managing her case?
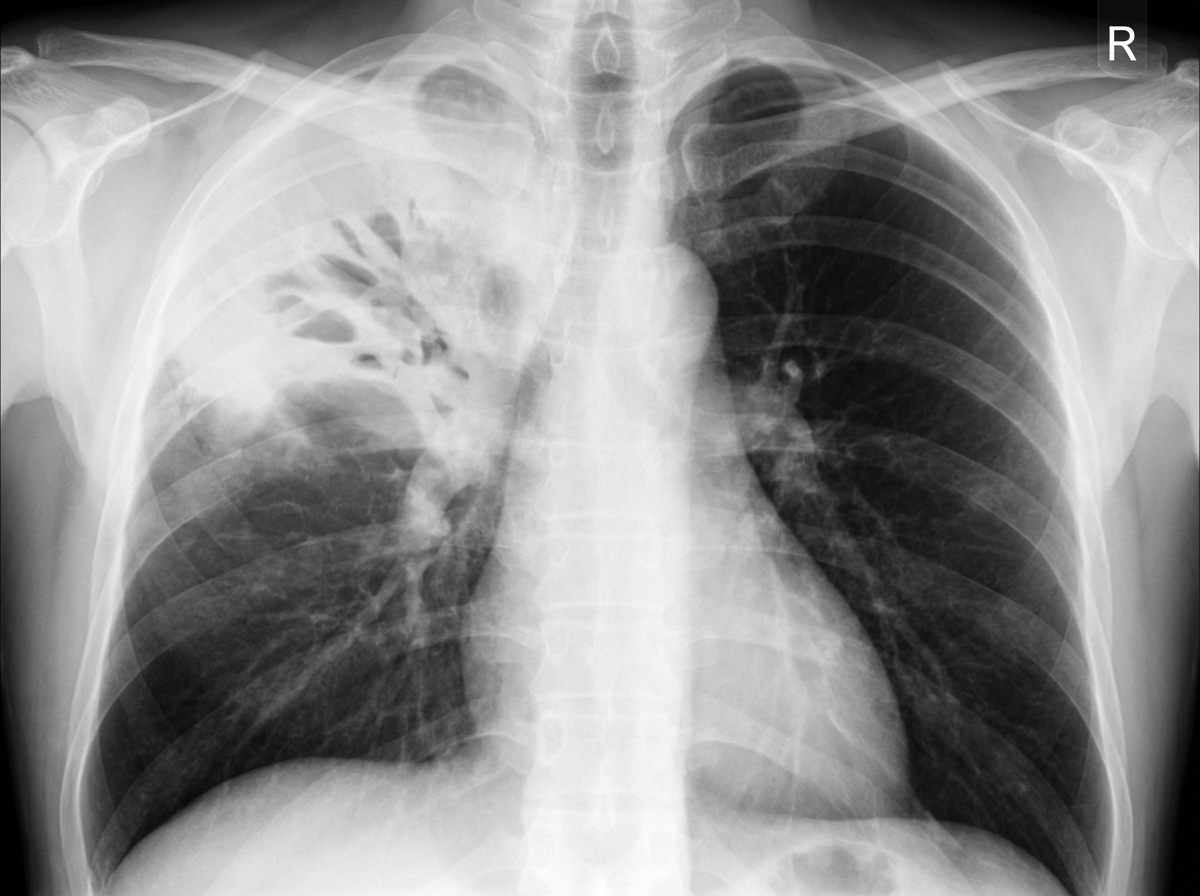
A 67-year-old woman is brought to the emergency department for evaluation of fever, chest pain, and a cough that has produced a moderate amount of greenish-yellow sputum for the past 2 days. During this period, she has had severe malaise, chills, and difficulty breathing. Her past medical history is significant for hypertension, hypercholesterolemia, and type 2 diabetes, for which she takes lisinopril, atorvastatin, and metformin. She has smoked one pack of cigarettes daily for 20 years. Her vital signs show her temperature is 39.0°C (102.2°F), pulse is 110/min, respirations are 33/min, and blood pressure is 143/88 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 94%. Crackles are heard on auscultation of the right upper lobe. Laboratory studies show a leukocyte count of 12,300/mm3, an erythrocyte sedimentation rate of 60 mm/h, and urea nitrogen of 15 mg/dL. A chest X-ray is shown, demonstrating right upper lobe consolidation with a cavitary lesion and air-fluid level, consistent with a lung abscess or cavitary pneumonia. Which of the following is the most appropriate next step to manage this patient's symptoms?
A 53-year-old woman presents to her primary care provider complaining of fatigue for the last several months. She reports feeling tired all day, regardless of her quality or quantity of sleep. On further questioning, she has also noted constipation and a 4.5 kg (10 lb) weight gain. She denies shortness of breath, chest pain, lightheadedness, or blood in her stool. At the doctor’s office, the vital signs include: pulse 58/min, blood pressure 104/68 mm Hg, and oxygen saturation 98% on room air. The physical exam shows only slightly dry skin. The complete blood count (CBC) is within normal limits. Which of the following best describes the pathogenesis of this patient's condition?
A 43-year-old man is brought to the emergency department because of severe retrosternal pain radiating to the back and left shoulder for 4 hours. The pain began after attending a farewell party for his coworker at a local bar. He had 3–4 episodes of nonbilious vomiting before the onset of the pain. He has hypertension. His father died of cardiac arrest at the age of 55 years. He has smoked one pack of cigarettes daily for the last 23 years and drinks 2–3 beers daily. His current medications include amlodipine and valsartan. He appears pale. His temperature is 37° C (98.6° F), pulse is 115/min, and blood pressure is 90/60 mm Hg. There are decreased breath sounds over the left base and crepitus is palpable over the thorax. Abdominal examination shows tenderness to palpation in the epigastric region; bowel sounds are normal. Laboratory studies show: Hemoglobin 16.5 g/dL Leukocyte count 11,100/mm3 Serum Na+ 133 mEq/L K+ 3.2 mEq/L Cl- 98 mEq/L HCO3- 30 mEq/L Creatinine 1.4 mg/dL An ECG shows sinus tachycardia with left ventricular hypertrophy. Intravenous fluid resuscitation and antibiotics are begun. Which of the following is the most appropriate test to confirm the diagnosis in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app