
Cardiology — MCQs

On this page
A 47-year-old woman comes to her primary care doctor because of a new, pruritic rash. She was gardening in her yard two days ago and now has an eczematous papulovesicular rash on both ankles. You also note a single, 5 mm brown lesion with a slightly raised border on her left thigh. You prescribe a topical corticosteroid for contact dermatitis. Which of the following is the appropriate next step for the thigh lesion?
A 45-year-old woman presents to her physician with a four-month history of headache. Her headache is nonfocal but persistent throughout the day without any obvious trigger. She was told that it was a migraine but has never responded to sumatriptan, oxygen, or antiemetics. She takes amlodipine for hypertension. She does not smoke. She denies any recent weight loss or constitutional symptoms. Her temperature is 98°F (36.7°C), blood pressure is 180/100 mmHg, pulse is 70/min, and respirations are 15/min. She is obese with posterior cervical fat pads and central abdominal girth. Her neurological exam is unremarkable. In her initial laboratory workup, her fasting blood glucose level is 200 mg/dL. The following additional lab work is obtained and is as follows: Serum: Na+: 142 mEq/L Cl-: 102 mEq/L K+: 4.1 mEq/L HCO3-: 24 mEq/L BUN: 20 mg/dL Glucose: 135 mg/dL Creatinine: 1.3 mg/dL Ca2+: 10.0 mg/dL AST: 8 U/L ALT: 8 U/L 24-hour urinary cortisol: 500 µg (reference range < 300 µg) Serum cortisol: 25 µg/mL (reference range 5-23 µg/dL) 24-hour low dose dexamethasone suppression test: Not responsive High dose dexamethasone suppression test: Responsive Adrenocorticotropin-releasing hormone (ACTH): 20 pg/mL (5-15 pg/mL) Imaging reveals a 0.5 cm calcified pulmonary nodule in the right middle lobe that has been present for 5 years but an otherwise unremarkable pituitary gland, mediastinum, and adrenal glands. What is the best next step in management?
A 23-year-old man presents to the emergency department brought in by police. He was found shouting at strangers in the middle of the street. The patient has no significant past medical history, and his only medications include a short course of prednisone recently prescribed for poison ivy exposure. His temperature is 77°F (25°C), blood pressure is 90/50 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. The patient is only wearing underwear, and he is occasionally mumbling angrily about the government. He appears to be responding to internal stimuli, and it is difficult to obtain a history from him. Which of the following is the next best step in management?
A 19-year-old man with a history of type 1 diabetes presents to the emergency department for the evaluation of a blood glucose level of 492 mg/dL. Laboratory examination revealed a serum bicarbonate level of 13 mEq/L, serum sodium level of 122 mEq/L, and ketonuria. Arterial blood gas demonstrated a pH of 6.9. He is admitted to the hospital and given bicarbonate and then started on an insulin drip and intravenous fluid. Seven hours later when his nurse is making rounds, he is confused and complaining of a severe headache. Repeat sodium levels are unchanged, although his glucose level has improved. His vital signs include a temperature of 36.6°C (98.0°F), pulse 50/min, respiratory rate 13/min and irregular, and blood pressure 177/95 mm Hg. What other examination findings would be expected in this patient?
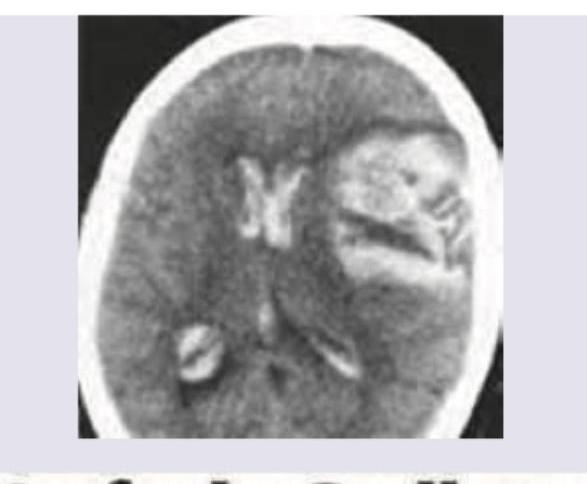
One day after undergoing a left carotid endarterectomy, a 63-year-old man has a severe headache. He describes it as 9 out of 10 in intensity. He has nausea. He had 80% stenosis in the left carotid artery and received heparin prior to the surgery. He has a history of 2 transient ischemic attacks, 2 and 4 months ago. He has hypertension, type 2 diabetes mellitus, and hypercholesterolemia. He has smoked one pack of cigarettes daily for 40 years. He drinks 1–2 beers on weekends. Current medications include lisinopril, metformin, sitagliptin, and aspirin. His temperature is 37.3°C (99.1°F), pulse is 111/min, and blood pressure is 180/110 mm Hg. He is confused and oriented only to person. Examination shows pupils that react sluggishly to light. There is a right facial droop. Muscle strength is decreased in the right upper and lower extremities. Deep tendon reflexes are 3+ on the right. There is a left cervical surgical incision that shows no erythema or discharge. Cardiac examination shows no abnormalities. A complete blood count and serum concentrations of creatinine, electrolytes, and glucose are within the reference range. A CT scan of the head is shown. Which of the following is the most important modifiable perioperative risk factor for this patient's condition?
A 25-year-old mother presents to her primary care physician for wrist pain. The patient recently gave birth to a healthy newborn at 40 weeks gestation. Beginning one week ago, she started having pain over her wrist that has steadily worsened. The patient notes that she also recently fell while walking and broke the fall with her outstretched arm. The patient is an accountant who works from home and spends roughly eight hours a day typing or preparing financial statements. Recreationally, the patient is a competitive cyclist who began a rigorous training routine since the birth of her child. The patient's past medical history is notable for hypothyroidism that is treated with levothyroxine. On physical exam, inspection of the wrist reveals no visible or palpable abnormalities. Pain is reproduced when the thumb is held in flexion, and the wrist is deviated toward the ulna. The rest of the patient's physical exam is within normal limits. Which of the following is the best next step in management?
A 61-year-old man presents to the urgent care clinic complaining of cough and unintentional weight loss over the past 3 months. He works as a computer engineer, and he informs you that he has been having to meet several deadlines recently and has been under significant stress. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type 2, and pulmonary histoplasmosis 10 years ago. He currently smokes 2 packs of cigarettes/day, drinks a 6-pack of beer/day, and he endorses a past history of cocaine use back in the early 2000s but currently denies any drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 18/min. His physical examination shows minimal bibasilar rales, but otherwise clear lungs on auscultation, grade 2/6 holosystolic murmur, and a benign abdominal physical examination. He appears euvolemic on exam. However, on routine lab testing, you notice that his sodium is 127 mEq/L, serum osmolality is 262 mOsm/kg (normal 275–295), urine osmolality is 480 mOsm/kg, and urine sodium is 42 mEq/L. His chest X-ray is shown in the picture. Which of the following is the most likely underlying diagnosis?

A 78-year-old man presents to the hospital because of shortness of breath and chest pain that started a few hours ago. 3 weeks ago he had surgery for a total hip replacement with a prosthesis. The patient was treated with prophylactic doses of low-molecular-weight heparin until he was discharged. He did not have a fever, expectoration, or any accompanying symptoms. He has a history of right leg deep vein thrombosis that occurred 5 years ago. His vital signs include: heart rate 110/min, respiratory rate 22/min, and blood pressure 150/90 mm Hg. There were no significant findings on the physical exam. Chest radiography was within normal limits. What is the most likely diagnosis?
A 74-year-old man is rushed to the emergency department with left-sided weakness, facial deviation, and slurred speech. His wife first noticed these changes about an hour ago. The patient is having difficulty communicating. He can answer questions by nodding his head, and his wife is providing detailed information. He denies fever, loss of consciousness, head injury, bleeding, or seizures. Past medical history is significant for diabetes mellitus, hypertension, hyperlipidemia, ischemic heart disease, chronic kidney disease, and osteoarthritis. He had a heart attack 6 weeks ago. Baseline creatinine is 2.5 mg/dL, and he is not on hemodialysis. Medications include aspirin, clopidogrel, metoprolol, ramipril, rosuvastatin, and insulin detemir. Blood pressure is 175/95 mm Hg and the heart rate is 121/min. Muscle strength is decreased in both the upper and lower extremities on the left-side. A forehead sparing left sided facial weakness is also appreciated. An ECG reveals atrial fibrillation. An urgent head CT shows a hypodense area in the right parietal cortex with no indication of hemorrhage. Treatment with tissue plasminogen activator (tPA) is deferred due to which condition?
A 45-year-old woman presents to her primary care provider complaining of daytime drowsiness and fatigue. She reports that she can manage at most a couple of hours of work before needing a nap. She has also noted impaired memory and a 6.8 kg (15 lb) weight gain. She denies shortness of breath, chest pain, lightheadedness, or blood in her stool. At the doctor’s office, the vital signs include: pulse 58/min, blood pressure 104/68 mm Hg, and oxygen saturation 99% on room air. The physical exam is notable only for slightly dry skin. The complete blood count (CBC) is within normal limits. Which of the following is a likely additional finding in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app