
Cardiology — MCQs

On this page
A 60-year-old lady presents with shortness of breath (SOB) and episodes of angina pectoris. Work-up reveals aortic stenosis. Which of the following is the most likely reason behind these chest pain episodes?
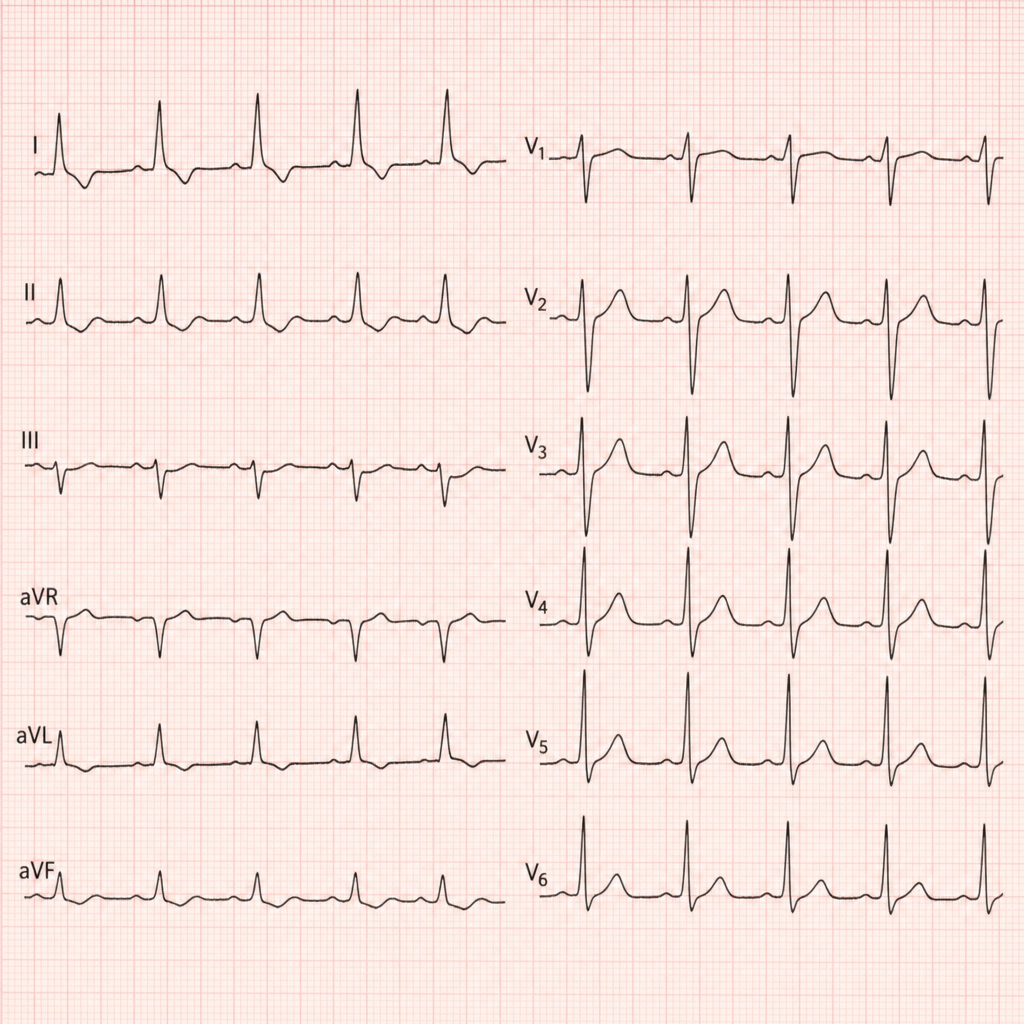
A patient with chronic kidney disease (CKD) presents with tachycardia, and the ECG is recorded as shown above. What is the most likely diagnosis?
A hypertensive patient presents with an irregularly irregular pulse and a loud P2 on auscultation. Which JVP finding is likely to be seen in this patient?
30-year-old male, weighing 70 kg , presents with a serum sodium level of $120 \mathrm{mEq} / \mathrm{L}$. Calculate the total sodium deficit.
A patient presents with confusion, altered mental status, and unusual behavior. On examination, CNS features such as disorientation and lethargy are noted. Laboratory results reveal a urine osmolality of 1000 mOsm/kg and a plasma osmolality of 250 mOsm/kg. What is the most likely electrolyte imbalance?
A patient presents with breathing difficulty and generalized weakness. On auscultation, a middiastolic murmur with a prominent "a" wave is observed. What is the most likely diagnosis?
A patient presents with breathlessness and wheezing. Absolute eosinophil count is 500 cells/ $\mu \mathrm{L}$. Chest X-ray shows a miliary pattern. What is the most likely diagnosis?
A 68-year-old male presents with cough, sputum production, bronchial breath sounds, respiratory rate of 20/min, urea of 44 mg/dl, and BP of 110/70 mmHg. What is the next step in management?
A known case of AIDS with a productive cough and fever is found to have consolidation in the right infrascapular area. Chest X-ray shows right lower lobe consolidation, and the CD4 count is 55 per microlitre. What is the most common cause of this presentation?
A patient presents with generalized and easy fatigability. He reports weakness while working in a factory with exposure to benzene. Which of the following conditions should be suspected in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app