
Cardiology — MCQs

On this page
A 55-year-old woman who is an established patient presents to your office. She is complaining of increased urination and increased thirst. She has recently began taking several over-the-counter vitamins and supplements. On further review, she reports she has also been having abdominal pain and constipation. She denies significant weight changes. Her fingerstick blood glucose in your office is 96 mg/dL. Which of the following test is most likely to provide the diagnosis?
A 15-year-old girl comes to the physician for a well-child examination. She feels well. Her father has coronary artery disease and hypertension. Her mother has type 2 diabetes mellitus, hypercholesterolemia, and had a myocardial infarction at the age of 52 years. She is at the 25th percentile for height and above the 95th percentile for weight. Her BMI is 32 kg/m2. Her temperature is 37°C (98.6°F), pulse is 99/min, and blood pressure is 140/88 mm Hg. Physical examination shows no abnormalities. Random serum studies show: Glucose 160 mg/dL Creatinine 0.8 mg/dL Total cholesterol 212 mg/dL HDL-cholesterol 32 mg/dL LDL-cholesterol 134 mg/dL Triglycerides 230 mg/dL In addition to regular aerobic physical activity, which of the following is the most appropriate next step in management?
A 39-year-old male is rushed to the emergency department after he developed a sudden-onset severe headache with ensuing nausea, vomiting, vision changes, and loss of consciousness. Past medical history is unattainable. He reports that the headache is worse than any he has experienced before. Noncontrast CT of the head is significant for an intracranial hemorrhage. Follow-up cerebral angiography is performed and shows a ruptured anterior communicating artery aneurysm. Which of the following has the strongest association with this patient's current presentation?
A 54-year-old man is brought to the emergency department because of progressive tingling and weakness in both of his legs for the past two days. The patient reports that his symptoms interfere with his ability to walk. Two weeks ago, he had an upper respiratory tract infection, which resolved spontaneously. His vital signs are within normal limits. Examination shows weakness in the lower extremities with absent deep tendon reflexes. Reflexes are 1+ in the upper extremities. Sensation to pinprick and light touch is intact. Romberg's test is negative. Laboratory studies show a leukocyte count of 12,000/mm3. Cerebrospinal fluid analysis results show: Opening pressure normal Protein 200 mg/dL Glucose 70 mg/dL White blood cells 4/mm3 This patient is at increased risk for which of the following conditions?
A 62-year-old Caucasian male presents to your office with hemoptysis and hematuria. On physical exam you note a saddle nose deformity. Laboratory results show an elevated level of cytoplasmic antineutrophil cytoplasmic antibody. Which of the following interventions is most appropriate for this patient?
A 5-year-old girl with an aortic stenosis correction comes to the office for a follow-up visit for acute lymphoblastic leukemia. She initiated chemotherapy a week before through a peripherally inserted central line. She reports being 'tired all the time' and has been bruising easily. Her vital signs are within normal limits. Physical examination shows several tender, non-blanching petechiae on the pads of the fingers and toes; several dark, non-tender petechiae on her palms and soles; and small, linear hemorrhages under her fingernails. Fundoscopic examination shows various small areas of hemorrhage on the retinae bilaterally. Cardiac examination is notable for a II/VI systolic ejection murmur that seems to have worsened in comparison to the last visit. Which of the following is the most likely cause?
A 57-year-old man comes to the physician because of a 2-month history of worsening shortness of breath with walking. He has not had any cough, fevers, or recent weight loss. He has hypercholesterolemia, for which he takes simvastatin, but otherwise is healthy. For 35 years he has worked for a demolition company. He has smoked 1 pack of cigarettes daily for the past 33 years. Pulmonary examination shows fine bibasilar end-expiratory crackles. An x-ray of the chest shows diffuse bilateral infiltrates predominantly in the lower lobes and bilateral calcified pleural plaques. The patient is most likely to develop which of the following conditions?
A 43-year-old woman presents to the physician with the complaint of worsening fatigue over the past several months. She has found that she requires nearly double the amount of coffee consumption each day to stay awake at work and that despite maintaining a balanced, healthy diet, she has experienced significant weight gain. A blood test confirms the presence of anti-thyroid peroxidase antibodies. Which of the following additional findings would be most consistent with the underlying pathophysiology of her condition?
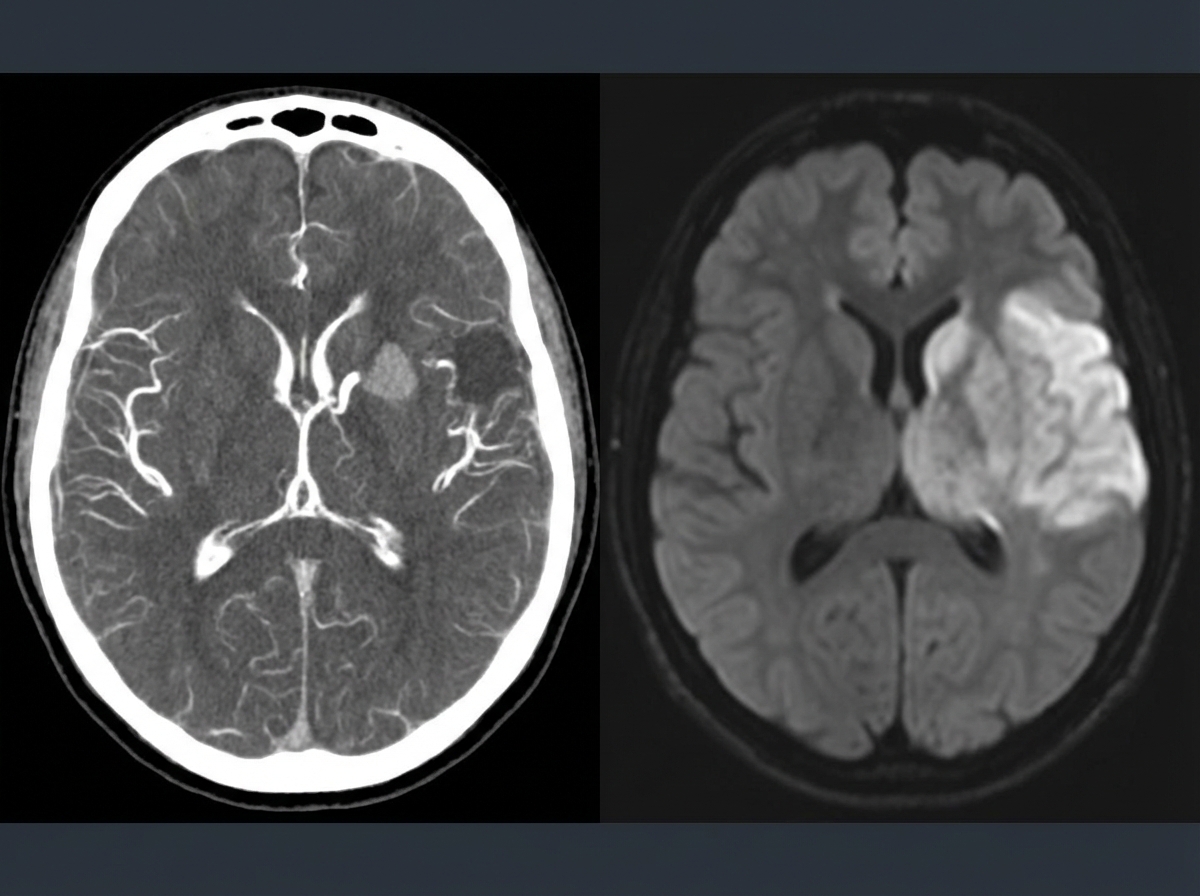
A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
A 48-year-old woman comes to the physician because of a 6-month history of muscle stiffness, myalgia, and a 7-kg (15-lb) weight gain. Her last menstrual period was 4 months ago. Physical examination shows cold, dry skin, and proximal muscle weakness. Deep tendon reflexes are 2+ bilaterally, with delayed relaxation. The creatine kinase level is 2,940 U/L. Which of the following is the most appropriate next step in diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app