
Cardiology — MCQs

On this page
A 37-year-old female presents to her primary care physician with constipation and abdominal pain. She notes that the pain has been present for several days and is not related to food. She also reports increased urinary frequency without incontinence, as well as increased thirst. She takes no medications, but notes taking vitamin supplements daily. Her vital signs are: BP 130/72 mmHg, HR 82 bpm, T 97.0 degrees F, and RR 12 bpm. Lab studies reveal: Na 139, K 4.1, Cl 104, HCO3 25, Cr 0.9, and Ca 12.4. Further studies show an increased ionized calcium, decreased PTH, and normal phosphate. What is the most likely cause of this patient's symptoms?
A 34-year-old woman is brought to the emergency department following a motor vehicle accident. She was walking on the sidewalk when a car traveling at high speed knocked her off her feet. She did not sustain any obvious injury but has painful breathing. An X-ray of the chest is taken to exclude a rib fracture and contusion of the lungs. The X-ray is found to be normal except for a solitary calcified nodule located in the left hilar region. The physician then asks the patient if she is or was a smoker, or has any pertinent medical history to explain the nodule. Her past medical history is insignificant, including any previous lung infections. Physical examination does not reveal any significant signs indicative of a tumor. A chest CT is ordered and a solitary nodule of 0.5 cm is confirmed. Which of the following is the most appropriate next step in the management of this patient?
A 13-year-old girl presents after losing consciousness during class 30 minutes ago. According to her friends, she was doing okay since morning, and nobody noticed anything abnormal. The patient’s mother says that her daughter does not have any medical conditions. She also says that the patient has always been healthy but has recently lost weight even though she was eating as usual. Her vital signs are a blood pressure of 100/78 mm Hg, a pulse of 89/min, and a temperature of 37.2°C (99.0°F). Her breathing is rapid but shallow. Fingerstick glucose is 300 mg/dL. Blood is drawn for additional lab tests, and she is started on intravenous insulin and normal saline. Which of the following HLA subtypes is associated with this patient’s most likely diagnosis?
A 58-year-old woman comes to the physician because of a 3-month history of recurring chest discomfort. The symptoms occur when walking up the stairs to her apartment or when walking quickly for 5 minutes on level terrain. She has not had shortness of breath, palpitations, or dizziness. She has hypertension and hyperlipidemia. Current medications include estrogen replacement therapy, metoprolol, amlodipine, lisinopril, hydrochlorothiazide, and rosuvastatin. She drinks 3–4 cups of coffee per day. She does not drink alcohol. Her pulse is 65/min, respirations are 21/min, and blood pressure is 145/90 mm Hg. Physical examination shows no abnormalities. A resting ECG shows normal sinus rhythm. She is scheduled for a cardiac exercise stress test in 2 days. Discontinuation of which of the following is the most appropriate next step in management at this time?
A 35-year-old woman with a medical history significant for asthma, hypertension, and occasional IV drug use comes to the emergency department with fever. On physical exam, there are findings depicted in figure A, for which the patient cannot account. What test will be most helpful to establish the diagnosis?

A previously healthy 21-year-old man is brought to the emergency department for the evaluation of an episode of unconsciousness that suddenly happened while playing football 30 minutes ago. He was not shaking and regained consciousness after about 30 seconds. Over the past three months, the patient has had several episodes of shortness of breath while exercising as well as sensations of a racing heart. He does not smoke or drink alcohol. He takes no medications. His vital signs are within normal limits. On mental status examination, he is oriented to person, place, and time. Cardiac examination shows a systolic ejection murmur that increases with valsalva maneuver and standing and an S4 gallop. The remainder of the examination shows no abnormalities. An ECG shows a deep S wave in lead V1 and tall R waves in leads V5 and V6. Echocardiography is most likely to show which of the following findings?
A 26-year-old woman presents with blood in her urine for the past 2 days. She says she has had increasing urinary frequency at night for the past several days and recently noticed a reddish tinge in her urine. She is also concerned that her feet are beginning to swell, and she has been feeling increasingly fatigued for the past week. She gives no history of joint pains, rashes, or skin changes. Past medical history is relevant for an occasional bluish discoloration of her fingers during exposure to cold. Her vital signs are a pulse of 80/min, a respiratory rate of 14/min, and blood pressure of 140/88 mm Hg. On physical examination, the patient has 1+ pitting edema of her feet bilaterally. Remainder of examination is unremarkable. Laboratory findings are significant for the following: Serum glucose (fasting) 88 mg/dL Sodium 143 mEq/L Potassium 3.7 mEq/L Chloride 102 mEq/L Serum creatinine 1.7 mg/dL Blood urea nitrogen 32 mg/dL Cholesterol, total 180 mg/dL HDL-cholesterol 43 mg/dL LDL-cholesterol 75 mg/dL Triglycerides 135 mg/dL Hemoglobin (Hb%) 12.5 g/dL Mean corpuscular volume (MCV) 80 fL Reticulocyte count 1% Erythrocyte count 5.1 million/mm3 Thyroid stimulating hormone 4.5 μU/mL Urinalysis: Glucose negative Protein +++ Ketones negative Nitrites negative RBCs negative Casts +++ A renal biopsy is performed which reveals findings consistent with lupus nephritis. Which of the following is the next best step in treatment of this patient?
A 66-year-old woman with no significant past medical, past surgical, or family history presents with new symptoms of chest pain, an oral rash, and pain with swallowing. She lost her husband several months earlier and has moved into an elderly assisted living community. She states that her symptoms began several weeks earlier. Physical examination reveals numerous white plaques on her buccal mucosa and tongue, raising suspicion for oral candidiasis. What is the next step in the patient’s management?
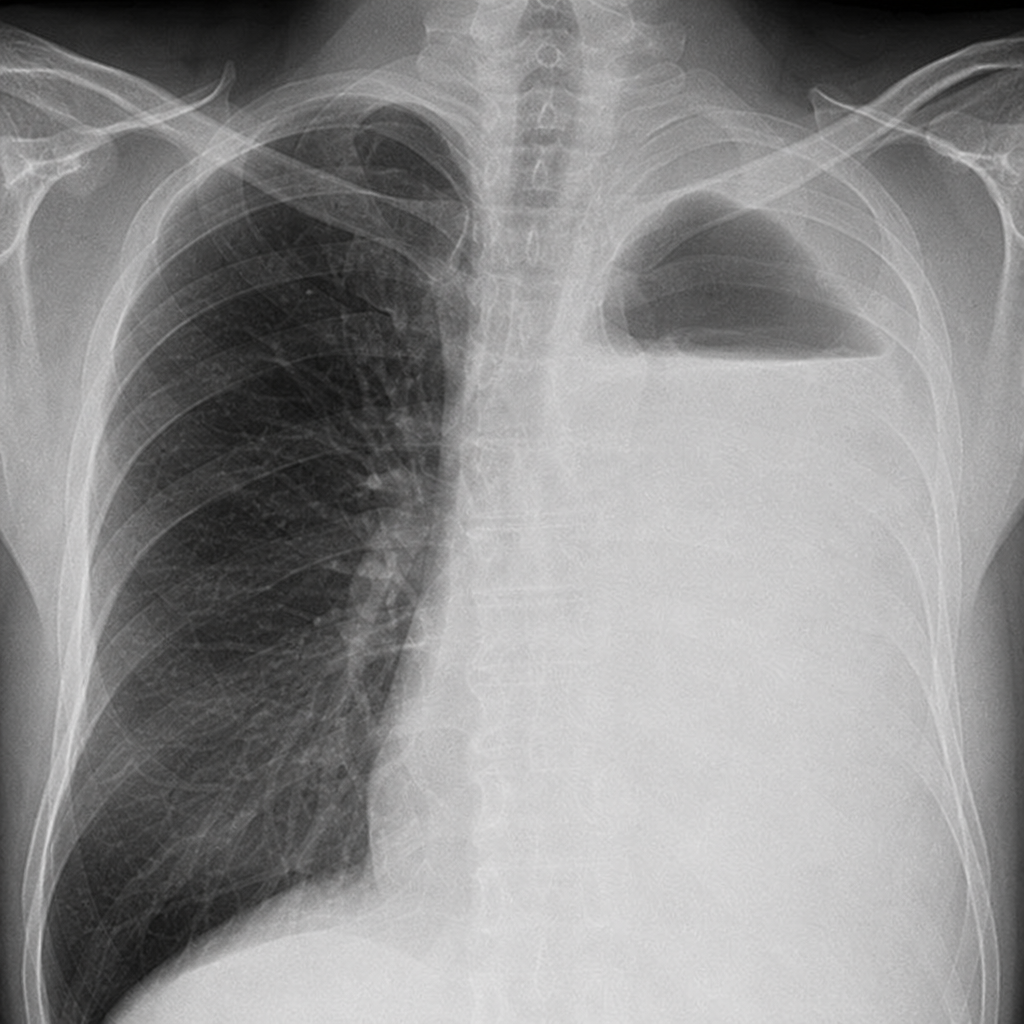
Six days after falling in the shower, a 75-year-old man with COPD is brought to the emergency department because of progressively worsening left-sided chest pain and shortness of breath. He has smoked one pack of cigarettes daily for 50 years. His temperature is 36.5°C (97.7°F), pulse is 110/min, respirations are 30/min, and blood pressure is 115/58 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 88%. Examination shows dullness to percussion and decreased fremitus over the left lung base. There are faint expiratory wheezes throughout the lungs. An x-ray of the chest is shown. Which of the following is the most likely cause of this patient’s current condition?
A 24-year-old man comes to the physician because of severe lower back pain for the past 2 days. The pain is constant and non-radiating, and he describes it as 7 out of 10 in intensity. The pain began after he helped a friend move into a new apartment. Three weeks ago, he was diagnosed with urethritis and was treated with azithromycin and ceftriaxone. He has a history of intravenous heroin use. He takes no medications. His temperature is 37°C (98.6°F), pulse is 98/min, and blood pressure is 128/90 mm Hg. Examination shows old track marks on the cubital fossae bilaterally. His lumbar paraspinal muscles are firm and tense on palpation. There is no midline spinal tenderness. Flexing the hip and extending the knee while raising the leg to 70° does not cause any pain. Urinalysis shows no abnormalities. Which of the following is the most appropriate next step in management?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app