
Cardiology — MCQs

On this page
Three days after undergoing open surgery to repair a bilateral inguinal hernia, a 66-year-old man has new, intermittent upper abdominal discomfort that worsens when he walks around. He also has new shortness of breath that resolves with rest. There were no complications during surgery or during the immediate postsurgical period. Ambulation was restarted on the first postoperative day. He has type 2 diabetes mellitus, hypercholesterolemia, and hypertension. He has smoked one pack of cigarettes daily for 25 years. Prior to admission, his medications included metformin, simvastatin, and lisinopril. His temperature is 37°C (98.6°F), pulse is 80/min, respirations are 16/min, and blood pressure is 129/80 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. The abdomen is soft and shows two healing surgical scars with moderate serous discharge. Cardiopulmonary examination shows no abnormalities. An ECG at rest shows no abnormalities. Cardiac enzyme levels are within the reference range. An x-ray of the chest and abdominal ultrasonography show no abnormalities. Which of the following is the most appropriate next step in diagnosis?
A 35-year-old woman who was recently ill with an upper respiratory infection presents to the emergency department with weakness in her lower limbs and difficulty breathing. Her symptoms began with a burning sensation in her toes along with numbness. She claims that the weakness has been getting worse over the last few days and now involving her arms and face. Currently, she is unable to get up from the chair without some assistance. Her temperature is 37.0°C (98.6°F), the blood pressure is 145/89 mm Hg, the heart rate is 99/min, the respiratory rate is 12/min, and the oxygen saturation is 95% on room air. On physical examination, she has diminished breath sounds on auscultation of bilateral lung fields with noticeably poor inspiratory effort. Palpation of the lower abdomen reveals a palpable bladder. Strength is 3 out of 5 symmetrically in the lower extremities bilaterally. The sensation is intact. What is the most likely diagnosis?
A 56-year-old woman presents with sudden-onset severe headache, nausea, vomiting, and neck pain for the past 90 minutes. She describes her headache as a ‘thunderclap’, followed quickly by severe neck pain and stiffness, nausea and vomiting. She denies any loss of consciousness, seizure, or similar symptoms in the past. Her past medical history is significant for an episode 6 months ago where she suddenly had trouble putting weight on her right leg, which resolved within hours. The patient denies any history of smoking, alcohol or recreational drug use. On physical examination, the patient has significant nuchal rigidity. Her muscle strength in the lower extremities is 4/5 on the right and 5/5 on the left. The remainder of the physical examination is unremarkable. A noncontrast CT scan of the head is normal. Which of the following is the next best step in the management of this patient?
A 72-year-old woman with hypertension comes to the physician because of swelling and pain in both legs for the past year. The symptoms are worse at night and improve in the morning. Current medications include losartan and metoprolol. Her temperature is 36°C (96.8°F), pulse is 67/min, and blood pressure is 142/88 mm Hg. Examination shows normal heart sounds; there is no jugular venous distention. Her abdomen is soft and the liver edge is not palpable. Examination of the lower extremities shows bilateral pitting edema and prominent superficial veins. The skin is warm and there is reddish-brown discoloration of both ankles. Laboratory studies show a normal serum creatinine and normal urinalysis. Which of the following is the most likely underlying cause of this patient's symptoms?
A 38-year-old woman presents with progressive muscle weakness. The patient says that symptoms onset a couple of weeks ago and have progressively worsened. She says she hasn't been able to lift her arms to comb her hair the past few days. No significant past medical history and no current medications. Family history is significant for her mother with scleroderma and an aunt with systemic lupus erythematosus (SLE). On physical examination, strength is 2 out of 5 in the upper extremities bilaterally. There is an erythematous area, consisting of alternating hypopigmentation and hyperpigmentation with telangiectasias, present on the extensor surfaces of the arms, the upper chest, and the neck in a 'V-shaped' distribution. Additional findings are presented in the exhibit (see image). Laboratory tests are significant for a positive antinuclear antibody (ANA) and elevated creatinine phosphokinase. Which of the following is the most appropriate first-line treatment for this patient?

A 50-year-old morbidly obese woman presents to a primary care clinic for the first time. She states that her father recently died due to kidney failure and wants to make sure she is healthy. She works as an accountant, is not married or sexually active, and drinks alcohol occasionally. She currently does not take any medications. She does not know if she snores at night but frequently feels fatigued. She denies any headaches but reports occasional visual difficulties driving at night. She further denies any blood in her urine or increased urinary frequency. She does not engage in any fitness program. She has her period every 2 months with heavy flows. Her initial vital signs reveal that her blood pressure is 180/100 mmHg and heart rate is 70/min. Her body weight is 150 kg (330 lb). On physical exam, the patient has droopy eyelids, a thick neck with a large tongue, no murmurs or clicks on cardiac auscultation, clear lungs, a soft nontender, albeit large abdomen, and palpable pulses in her distal extremities. She can walk without difficulty. A repeat measurement of her blood pressure shows 155/105 mmHg. Which among the following is part of the most appropriate next step in management?
A 32-year-old woman comes to the physician because of a 4-day history of low-grade fever, joint pain, and muscle aches. The day before the onset of her symptoms, she was severely sunburned on her face and arms during a hike with friends. She also reports being unusually fatigued over the past 3 months. Her only medication is a combined oral contraceptive pill. Her temperature is 37.9°C (100.2°F). Examination shows bilateral swelling and tenderness of the wrists and metacarpophalangeal joints. There are multiple nontender superficial ulcers on the oral mucosa. The detection of antibodies directed against which of the following is most specific for this patient's condition?
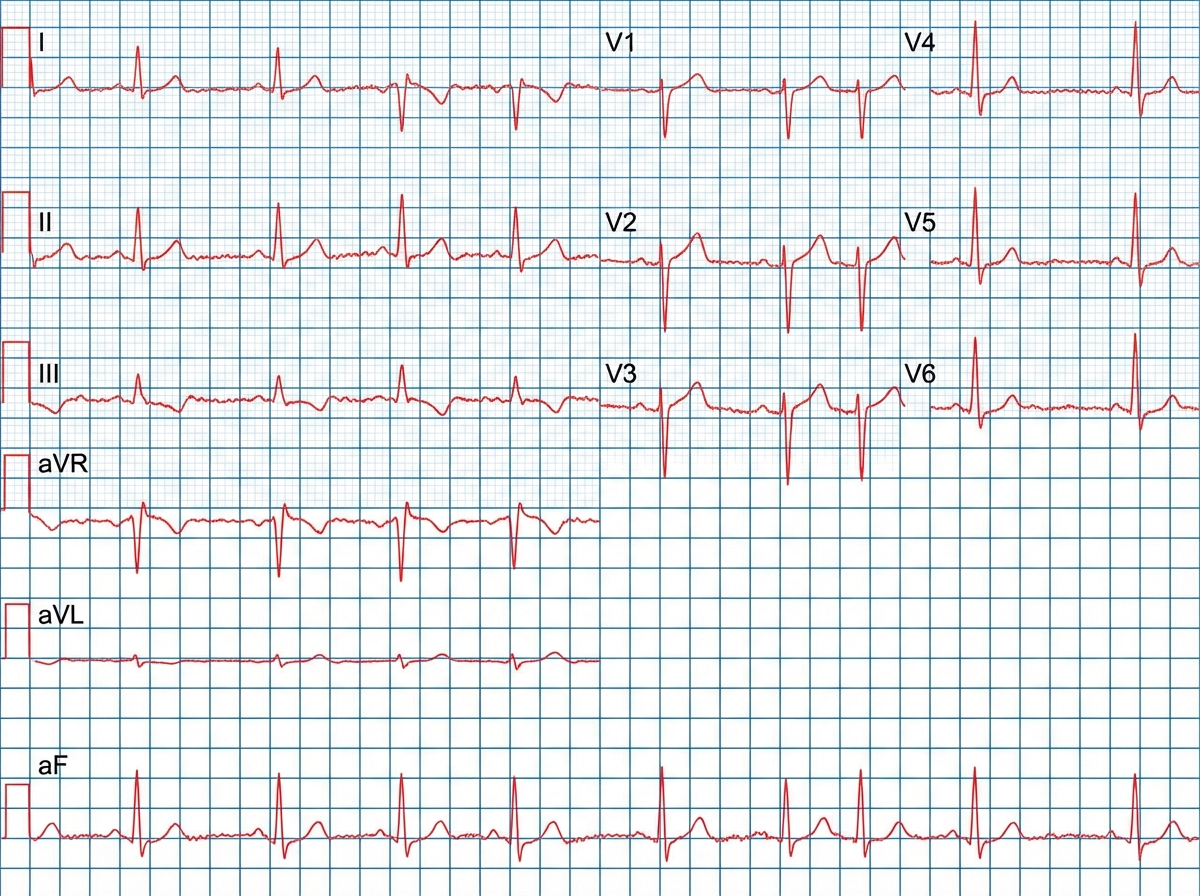
A 67-year-old woman comes to the physician because of intermittent chest pain and dizziness on exertion for 6 months. Her pulse is 76/min and blood pressure is 125/82 mm Hg. Cardiac examination shows a grade 3/6, late-peaking, crescendo-decrescendo murmur heard best at the right upper sternal border. An echocardiogram confirms the diagnosis. Three months later, the patient returns to the physician with worsening shortness of breath for 2 weeks. An ECG is shown. Which of the following changes is most likely responsible for this patient's acute exacerbation of symptoms?
A 67-year-old man presents to his primary care physician complaining of frequent urination overnight. He states that for several years he has had trouble maintaining his urine stream along with the need for frequent urination, but the nighttime urination has only recently started. The patient also states that he has had 2 urinary tract infections in the last year, which he had never had previously. On exam, his temperature is 98.8°F (37.1°C), blood pressure is 124/68 mmHg, pulse is 58/min, and respirations are 13/min. On digital rectal exam, the prostate is enlarged but feels symmetric and smooth. Which of the following is a possible consequence of this condition?
A 49-year-old male presents with a primary complaint of several recent episodes of severe headache, sudden anxiety, and a "racing heart". The patient originally attributed these symptoms to stress at work; however, these episodes are becoming more frequent and severe. Laboratory evaluation during such an episode reveals elevated plasma free metanephrines. Which of the following additional findings in this patient is most likely?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app