
Cardiology — MCQs

On this page
A 66-year-old man is brought into the emergency department by his daughter for a change in behavior. Yesterday the patient seemed more confused than usual and was asking the same questions repetitively. His symptoms have not improved over the past 24 hours, thus the decision to bring him in today. Last year, the patient was almost completely independent but he then suffered a "series of falls," after which his ability to care for himself declined. After this episode he was no longer able to cook for himself or pay his bills but otherwise had been fine up until this episode. The patient has a past medical history of myocardial infarction, hypertension, depression, diabetes mellitus type II, constipation, diverticulitis, and peripheral neuropathy. His current medications include metformin, insulin, lisinopril, hydrochlorothiazide, sodium docusate, atorvastatin, metoprolol, fluoxetine, and gabapentin. On exam you note a confused man who is poorly kept. He has bruises over his legs and his gait seems unstable. He is alert to person and place, and answers some questions inappropriately. The patient's pulse is 90/minute and his blood pressure is 170/100 mmHg. Which of the following is the most likely diagnosis?
A 33-year-old African American woman presents to the office complaining of blurry vision and headache for the past 2 weeks. She states that she has not been feeling herself lately and also fell down once after a dizzy episode. Her medical history is remarkable for hypertension and pulmonary sarcoidosis treated with hydralazine and prednisone respectively. She had a recent bout of acute optic neuritis, requiring high-dose IV methylprednisolone. Her temperature is 37°C (98.6°F), the blood pressure is 112/76 mm Hg, the pulse is 78/min, and the respirations are 14/min. On examination, the patient is mildly disoriented. Head and neck examination reveals a soft, supple neck and a right-sided facial droop. There is 5/5 muscle strength in all extremities. VDRL test is negative. A head MRI is pending. What is the most appropriate next step in the management of this patient?
A 74-year-old man presents to the emergency department by paramedics for slurred speech and weakness in the left arm and leg for 1 hour. The patient was playing with his grandson when the symptoms started and his wife immediately called an ambulance. There is no history of head trauma or recent surgery. The patient takes captopril for hypertension. The vital signs include: pulse 110/min, respiratory rate 22/min, and blood pressure 200/105 mm Hg. The physical examination shows that the patient is alert and conscious, but speech is impaired. Muscle strength is 0/5 in the left arm and leg and 5/5 in the right arm and leg. A non-contrast CT of the head shows no evidence of intracranial bleeding. The lab results are as follows: Serum glucose 90 mg/dL Sodium 140 mEq/L Potassium 4.1 mEq/L Chloride 100 mEq/L Serum creatinine 1.3 mg/dL Blood urea nitrogen 20 mg/dL Cholesterol, total 240 mg/dL HDL-cholesterol 38 mg/dL LDL-cholesterol 100 mg/dL Triglycerides 190 mg/dL Hemoglobin (Hb%) 15.3 g/dL Mean corpuscular volume (MCV) 83 fL Reticulocyte count 0.8% Erythrocyte count 5.3 million/mm3 Platelet count 130,000/mm3 Partial thromboplastin time (aPTT) 30 sec Prothrombin time (PT) 12 sec Although he is within the time frame for the standard therapy of the most likely condition, the treatment cannot be started because of which of the following contraindications?
A 40-year-old man comes to the physician because of a 2-year history of gradually worsening shortness of breath. He smoked half a pack of cigarettes daily for 10 years but stopped 8 years ago. His pulse is 72/min, blood pressure is 135/75 mm Hg, and respirations are 20/min. Examination shows an increased anteroposterior diameter of the chest. Diminished breath sounds are heard on auscultation of the chest. An x-ray of the chest shows widened intercostal spaces, a flattened diaphragm, and bilateral hyperlucency of the lung bases. This patient's condition puts him at greatest risk for which of the following conditions?
A 45-year-old man presents to the emergency department with decreased exercise tolerance and shortness of breath which has progressed slowly over the past month. The patient recalls that shortly before the onset of these symptoms, he had a low-grade fever, malaise, and sore throat which resolved after a few days with over the counter medications. He does not have any chronic illnesses and denies recent travel or illicit habits. His vital signs include: blood pressure 120/80 mm Hg, temperature 37.0°C (98.6°F), and regular radial pulse 90/min. While checking his blood pressure manually, the difference between the systolic pressure at which the first Korotkoff sounds are heard during expiration and the pressure at which they are heard throughout the respiratory cycle is less than 10 mm Hg. On physical examination, he is in mild distress with jugular venous pressure (JVP) of 13 cm, and his heart sounds are muffled. His echocardiography shows a fluid collection in the pericardial sac with no evidence of right ventricular compression. Which of the following is the best initial step for the treatment of this patient?
A 51-year-old woman presents for her annual wellness visit. She says she feels healthy and has no specific concerns. Past medical history is significant for bipolar disorder, hypertension, and diabetes mellitus type 2, managed with lithium, lisinopril, and metformin, respectively. Her family history is significant for hypertension and diabetes mellitus type 2 in her father, who died from lung cancer at age 67. Her vital signs include: temperature 36.8°C (98.2°F), pulse 97/min, respiratory rate 16/min, blood pressure 120/75 mm Hg. Physical examination is unremarkable. Mammogram findings are labeled breast imaging reporting and data system-3 (BIRADS-3) (probably benign). Which of the following is the next best step in management in this patient?
A 35-year-old woman presents as a new patient to a primary care physician. She hasn't seen a doctor in many years and came in for a routine check-up. She has no specific complaints, although she has occasional shortness of breath with mild activity. On physical exam, her vital signs are as follows: HR 80, BP 110/70, RR 14. On auscultation, her lungs are clear with equal breath sounds bilaterally. When listening over the precordium, the physician hears a mid-systolic click followed by a late systolic murmur that is loudest over the apex. Valsalva increases the murmur. Which of the following is NOT a possible complication of this patient's underlying problem?
A 62-year-old man comes to the physician because of a 5-day history of swelling in his left arm. Two months ago, he was diagnosed with a deep venous thrombosis in the left calf. He has had a 7-kg (15-lb) weight loss in the last 3 months. He has smoked 1 pack of cigarettes daily for the past 25 years. His only medication is warfarin. Physical examination shows warm edema of the left forearm with overlying erythema and a tender, palpable cord-like structure along the medial arm. His lungs are clear to auscultation bilaterally. Duplex sonography shows thrombosis of the left basilic and external jugular veins. Which of the following is the most appropriate next step to confirm the underlying diagnosis?
A 28-year-old woman presents to the emergency department with fever, cough, and difficulty in breathing for the last 6 hours. She also mentions that she noticed some blood in her sputum an hour ago. She denies nasal congestion or discharge, sneezing, wheezing, chest pain, or palpitation. Her past history does not suggest any chronic medical condition, including respiratory disease, cardiovascular disease, or cancer. There is no history of pulmonary embolism or deep vein thrombosis in the past. Her temperature is 38.3°C (101.0°F), the pulse is 108/min, the blood pressure is 116/80 mm Hg, and the respirations are 28/min. Auscultation of her lungs reveals the presence of localized crackles over the right inframammary region. Edema is present over her left leg and tenderness is present over her left calf region. When her left foot is dorsiflexed, she complains of calf pain. The emergency department protocol mandates the use of a modified Wells scoring system in all patients presenting with the first episode of breathlessness when there is no history of a cardiorespiratory disorder in the past. According to the modified Wells scoring system, which of the following risk factors, if present, would contribute the most points toward a high clinical probability of pulmonary embolism?
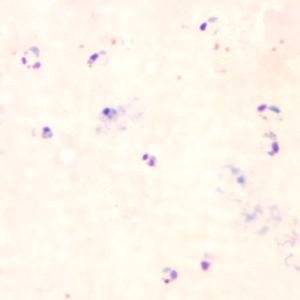
A 30-year-old woman seeks evaluation at a clinic complaining of shaking, chills, fevers, and headaches for the last 3 days. She recently returned from a trip to India, where she was visiting her family. There is no history of loss of consciousness or respiratory distress. The vital signs include temperature 38.9℃ (102.0℉), respiratory rate 19/min, blood pressure 120/80 mm Hg, and pulse 94/min (rapid and thready). On general examination, she is pale and the sclera is jaundiced. Laboratory studies show: Hematocrit (Hct) 30% Total bilirubin 2.6 mg/dL Direct bilirubin 0.3 mg/dL A peripheral smear is shown below. What is the most severe complication of this condition?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app