
Cardiology — MCQs

On this page
A 72-year-old man is brought to the emergency department after an episode of hemoptysis. He has a chronic cough that is productive of copious sputum. Six years ago, he had a stroke that left him with difficulty swallowing. He smoked one pack of cigarettes daily for 40 years, but quit 2 years ago. His respirations are 25/min and labored. Physical examination shows digital clubbing. An x-ray of the chest shows tram track opacities in the lower lung fields. Which of the following is the most likely diagnosis?
A 48-year-old male presents to his primary physician with the chief complaints of fever, abdominal pain, weight loss, muscle weakness, and numbness in his lower extremities. UA is normal. A biopsy of the sural nerve reveals transmural inflammation and fibrinoid necrosis of small and medium arteries. Chart review reveals a remote history of cigarette smoking as a teenager and Hepatitis B seropositivity. What is the most likely diagnosis?
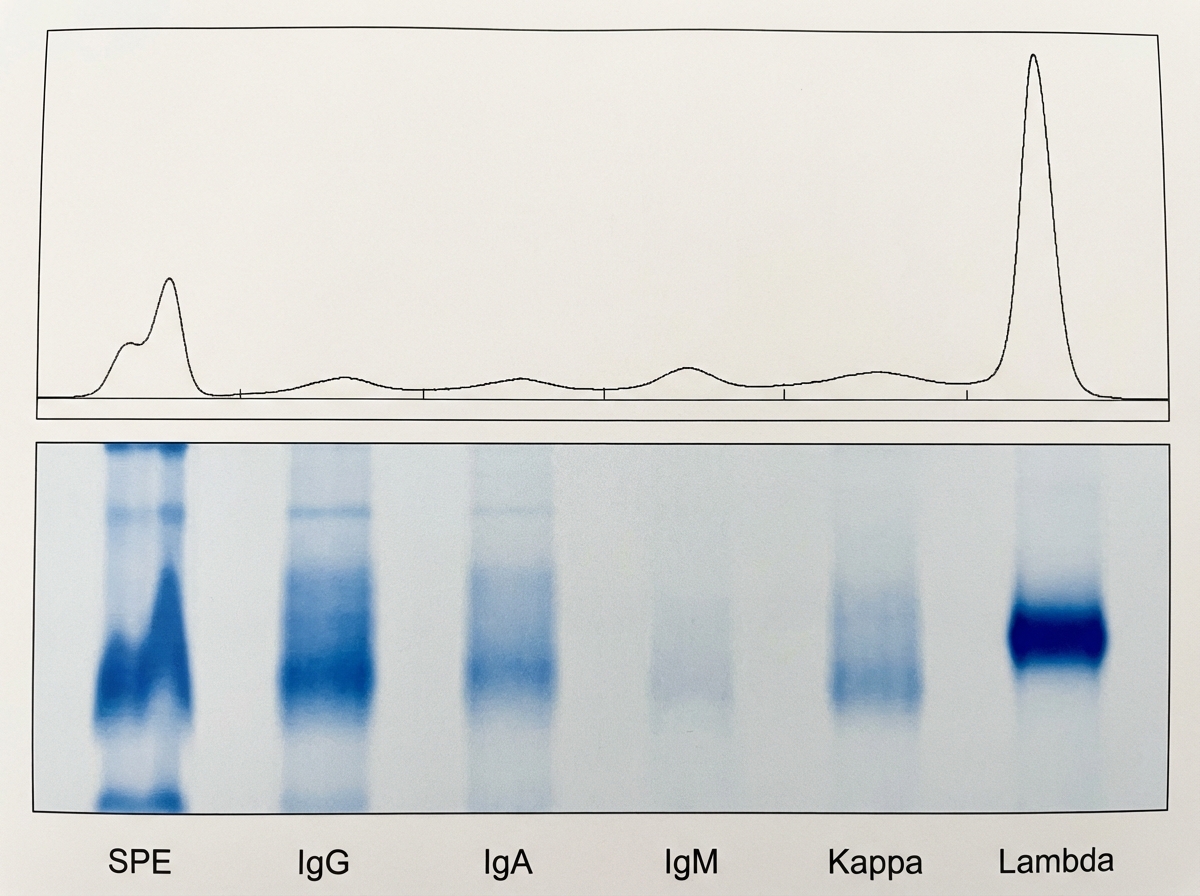
A 71-year-old man comes to the physician for a health maintenance examination. Aside from occasional lower back pain in the last couple of years, he feels well. He had a right-sided myocardial infarction 4 years ago. Currently, he has no shortness of breath and has no anginal symptoms. He has a 30 pack-year history of smoking but stopped smoking 10 years ago and does not drink alcohol. His pulse is 59/min, and his blood pressure is 135/75 mm Hg. Physical examination reveals 1+ lower extremity edema. Cardiac and pulmonary auscultation show no abnormalities. There is no lymphadenopathy. His laboratory studies show a hemoglobin of 13.2 g/dL and serum protein of 10.1 g/dL. ECG shows known Q wave abnormalities unchanged since the last ECG one year ago. A serum protein electrophoresis with immunofixation is shown. Which of the following is the most appropriate next step to establish the diagnosis?
A previously healthy 64-year-old woman comes to the physician because of a dry cough and progressively worsening shortness of breath for the past 2 months. She has not had fever, chills, or night sweats. She has smoked one pack of cigarettes daily for the past 45 years. She appears thin. Examination of the lung shows a prolonged expiratory phase and end-expiratory wheezing. Spirometry shows decreased FEV1:FVC ratio (< 70% predicted), decreased FEV1, and a total lung capacity of 125% of predicted. The diffusion capacity of the lung (DLCO) is decreased. Which of the following is the most likely diagnosis?
A 63-year-old man comes to the physician because of a 2-day history of a painful rash on his right flank. Two years ago, he underwent cadaveric renal transplantation. Current medications include tacrolimus, mycophenolate mofetil, and prednisone. Examination shows an erythematous rash with grouped vesicles in a band-like distribution over the patient's right flank. This patient is at greatest risk for which of the following complications?
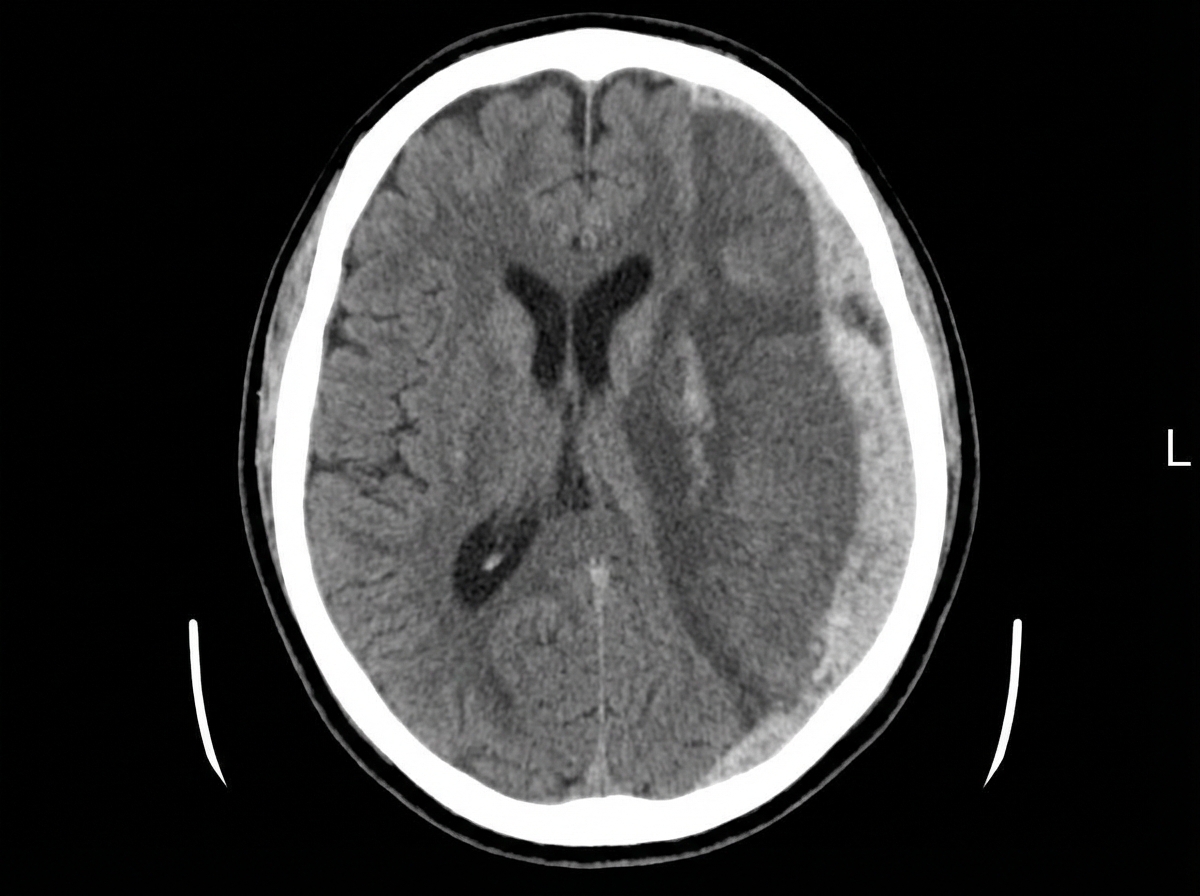
A 68-year-old man is brought to the emergency department by his wife because of a 2-week history of progressive disorientation and a 1-day history of left-sided weakness and difficulty speaking. The wife reports that the patient had a minor fall 4 months ago, during which he may have hit his head. He has hypertension and hyperlipidemia. He drinks 3–4 bottles of beer daily. He is only oriented to person. Neurological examination shows moderate spastic weakness, decreased sensation, and increased deep tendon reflexes in the left upper and lower extremities. A CT scan of the head is shown. Which of the following is the most likely cause of this patient's condition?
A 23-year-old female presents to the emergency department with monocular blindness. She states that early this morning she lost her vision seemingly "out of nowhere." She denies trauma or any precipitating factors. She does state though that over the past year she has had occasional episodes of weakness and even an episode of urinary incontinence, which always resolve on their own. On exam, pain is elicited with eye movement and nystagmus is appreciated. The emergency physician performs a lumbar puncture. What is most likely to be observed in the CSF of this patient?
A 52-year-old man presents to his primary care physician to discuss laboratory results that were obtained during his annual checkup. He has no symptoms or concerns and denies changes in eating or urination patterns. Specifically, the physician ordered a panel of metabolic laboratory tests to look for signs of diabetes, hyperlipidemia, or other chronic disorders. A spot glucose check from a random blood sample showed a glucose level of 211 mg/dL. A hemoglobin A1c level was obtained at the same time that showed a level of 6.3%. A fasting blood glucose was obtained that showed a blood glucose level of 125 mg/dL. Finally, a 2-hour glucose level was obtained after an oral glucose tolerance test that showed a glucose level of 201 mg/dL. Which of the following statements is most accurate for this patient?
A 32-year-old woman presents to the clinic with the complaint of excessive fatigue for the past few weeks. After returning home from the office, she feels too tired to climb up the stairs, comb her hair, or chew her food. She has occasionally experienced double vision. She denies any history of fever, cough, weight loss, night sweats, or snoring. Past history is unremarkable. Physical examination reveals: blood pressure 124/86 mm Hg, heart rate 85/min, respiratory rate 14/min, temperature 37.0°C (98.6°F), and body mass index (BMI) 22.6 kg/m2. On examination, the right upper eyelid is slightly drooping when compared to the left side. Her eye movements are normal. Flexion of the neck is mildly weak. Muscle strength is 5/5 in all 4 limbs. When she is asked to alternately flex and extend her shoulder continuously for 5 minutes, the power in the proximal upper limb muscles becomes 4/5. The muscle tone and deep tendon reflexes are normal. What is the most appropriate test to diagnose this condition?
A 25-year-old woman presents into the clinic complaining of worsening malaise, hair loss, and a rash on her face. The patient states that she has been avoiding daylight because the rash becomes painful, and she has not been able to go to classes because of debilitating arthralgia in her fingers and ankles. No significant past medical history. She takes no medication. At the time of the consult, the patient has a fever of 39.0°C (102.2 °F). The presence of which of the following is most commonly seen on diagnostic labs in this patient’s most likely condition?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app