
Cardiology — MCQs

On this page
A patient presents with features of heart failure. On examination, an irregularly irregular pulse is noted, and the patient has a loud diastolic sound. The jugular venous pressure (JVP) shows a rapid Y descent. What is the most likely diagnosis?
A 35-year-old male from a rural village in South Asia is admitted to the hospital with a 5-day history of high-grade fever, severe headache, and progressive breathlessness. His family reports that he has become increasingly disoriented over the past 48 hours, with episodes of confusion and drowsiness. Upon examination, the patient is febrile with a temperature of 39°C (102.2°F), tachypneic with a respiratory rate of 30 breaths per minute, and is displaying signs of altered mental status, including lethargy and difficulty following commands. His oxygen saturation is 92% on room air. There are no signs of a rash or bleeding. What is the diagnosis?
A 32-year-old female presents with a 2-month history of progressive, painless swelling in the left side of her neck. She also reports low-grade fever, night sweats, and unintentional weight loss. Physical examination reveals a firm, non-tender, immobile mass in the left cervical region, and multiple smaller lymph nodes in the supraclavicular area. Chest X-ray shows mediastinal widening, and a lymph node biopsy confirms the presence of Reed-Sternberg cells. What is the most appropriate management for this patient?
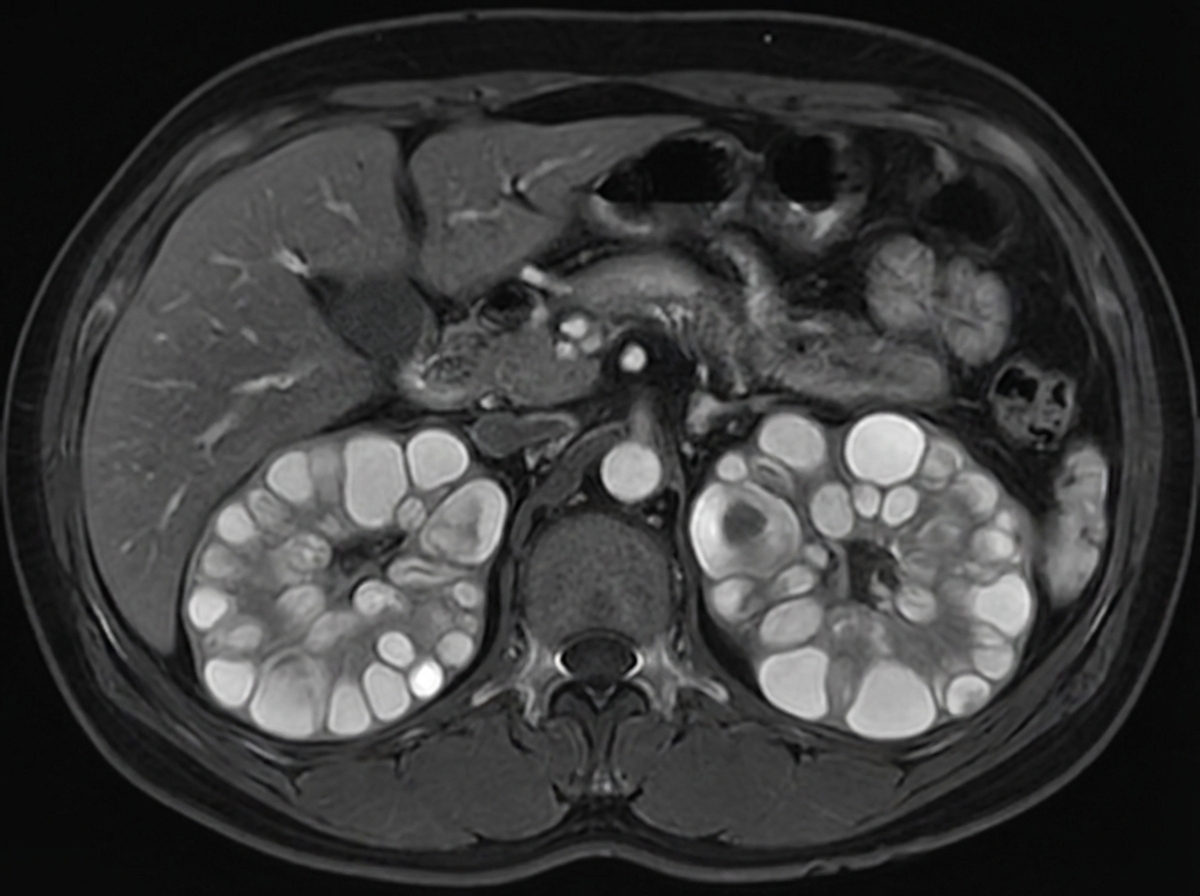
A 45-year-old patient presents with hypertension, hematuria, and flank pain. An MRI scan is performed, and the image provided shows multiple cystic lesions in both kidneys. What is the most likely diagnosis?
A patient presents with large sweaty hands, macroglossia, and frontal bossing. What is the best test for confirmation of the diagnosis?
What is the most common cause of death in idiopathic pulmonary fibrosis (IPF)?
In Type 1 Diabetes Mellitus (DM) stage 3 beta cell destruction, which of the following is the most likely presentation?
A young patient in an endemic area presents with pleural fluid showing LDH level greater than 0.6 times the serum LDH, protein level greater than 0.5 times the serum protein, and lymphocytic predominance. What is the most likely diagnosis?
A patient presents with hypotension, hyponatremia, and blackening of the palmar creases. Which of the following conditions is most likely associated with these symptoms?
A patient presents with wheezing that improves with as-needed use of albuterol. Spirometry shows FEV1 ranging from 70 % to 83 %, and the patient experiences nighttime chest tightening twice a week. What is the most appropriate treatment?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app