
Cardiology — MCQs

On this page
A 55-year-old man presents to the emergency department for chest pain. He states that the pain started last night and has persisted until this morning. He describes the pain as in his chest and radiating into his back between his scapulae. The patient has a past medical history of alcohol abuse and cocaine abuse. He recently returned from vacation on a transatlantic flight. The patient has smoked 1 pack of cigarettes per day for the past 20 years. His temperature is 99.5°F (37.5°C), blood pressure is 167/118 mmHg, pulse is 120/min, and respirations are 22/min. Physical exam reveals tachycardia and clear air movement bilaterally on cardiopulmonary exam. Which of the following is also likely to be found in this patient?
A 67-year old woman is brought to the emergency department after she lost consciousness while at home. Her daughter was with her at the time and recalls that her mother was complaining of a diffuse headache and nausea about 2 hours before the incident. The daughter says that her mother has not had any recent falls and was found sitting in a chair when she lost consciousness. She has hypertension. Current medications include amlodipine, a daily multivitamin, and acetaminophen. She has smoked 1/2 pack of cigarettes daily for the past 45 years. Her pulse is 92/min, respirations are 10/min, and blood pressure is 158/100 mm Hg. She is disoriented and unable to follow commands. Examination shows nuchal rigidity. She has flexor posturing to painful stimuli. Fundoscopic examination is notable for bilateral vitreous hemorrhages. Laboratory studies are within normal limits. An emergent non-contrast CT scan of the head is obtained and shows a diffuse hemorrhage at the base of the brain that is largest over the left hemisphere. Which of the following is the most likely cause of this patient's symptoms?
A 33-year-old woman comes to the physician because of left leg pain and swelling for 1 day. She has had two miscarriages but otherwise has no history of serious illness. Physical examination shows stiff, swollen finger joints. The left calf circumference is larger than the right and there is a palpable cord in the left popliteal fossa. Laboratory studies show a prothrombin time of 12 seconds and an activated partial thromboplastin time of 51 seconds. Which of the following is most likely to confirm the diagnosis?
A 57-year-old man comes to the physician two weeks after a blood pressure of 160/92 mm Hg was measured at a routine health maintenance examination. Subsequent home blood pressure measurements since the last visit have been: 159/98 mm Hg, 161/102 mm Hg, and 152/95 mm Hg. Over the past 3 years, the patient has had a 10-kg (22-lb) weight gain. He has type 2 diabetes mellitus. He does not follow any specific diet; he usually eats sandwiches at work and fried chicken or burger for dinner. He says that he has been struggling with a stressful project at work recently. His mother was diagnosed with hypertension at the age of 45. The patient's only medication is metformin. His pulse is 82/min, and blood pressure now is 158/98 mm Hg. The patient is 178 cm (5 ft 10 in) tall and weighs 133 kg (293 lb); BMI is 42 kg/m2. Physical examination shows no other abnormalities except for significant central obesity. Fasting serum studies show: Total cholesterol 220 mg/dL HDL-cholesterol 25 mg/dL Triglycerides 198 mg/dL Glucose 120 mg/dL Which of the following is the most important factor in the development of this patient's condition?
A 67-year-old man is brought to the emergency department because of increasing shortness of breath that began while playing outdoors with his grandson. He has a history of asthma but does not take any medications for it. On arrival, he is alert and oriented. He is out of breath and unable to finish his sentences. His pulse is 130/min, respirations are 23/min and labored, and blood pressure is 110/70 mm Hg. Physical examination shows nasal flaring and sternocleidomastoid muscle use. Pulmonary exam shows poor air movement bilaterally but no wheezing. Cardiac examination shows no abnormalities. Oxygen is administered via non-rebreather mask. He is given three albuterol nebulizer treatments, inhaled ipratropium, and intravenous methylprednisolone. The patient is confused and disoriented. Arterial blood gas analysis shows: pH 7.34 Pco2 44 mm Hg Po2 54 mm Hg O2 saturation 87% Which of the following is the most appropriate next step in management?
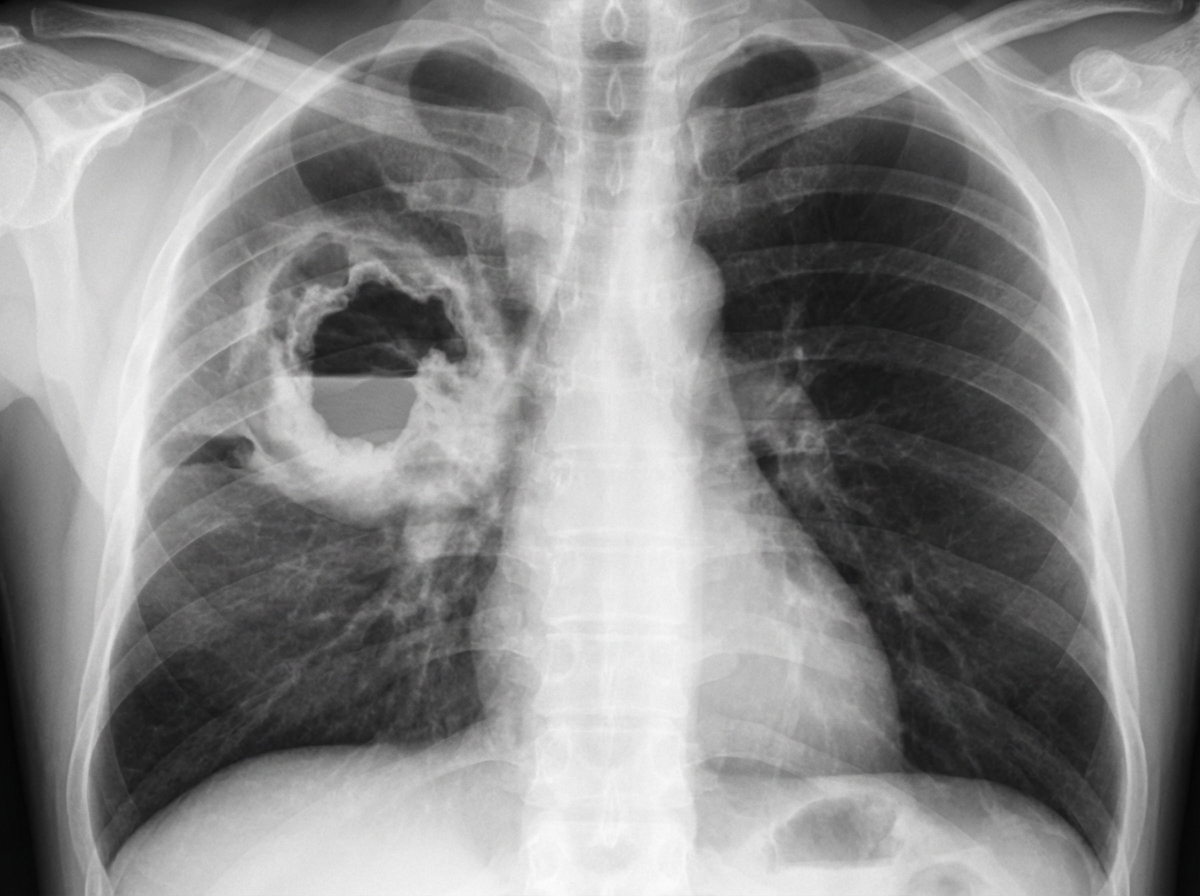
A 65-year-old woman presents to her physician with a persistent and debilitating cough which began 3 weeks ago, and chest pain accompanied by shortness of breath for the past week. Past medical history is significant for breast carcinoma 10 years ago treated with mastectomy, chemotherapy and radiation, a hospitalization a month ago for pneumonia that was treated with antibiotics, hypertension, and diabetes mellitus. Medications include chlorthalidone and metformin. She does not smoke but her husband has been smoking 3 packs a day for 30 years. Today her respiratory rate is 20/min and the blood pressure is 150/90 mm Hg. Serum Na is 140 mmol/L, serum K is 3.8 mmol/L and serum Ca is 12.2 mg/dL. A chest X-ray (shown in image) is performed. Which of the following is the most likely diagnosis?
A 25-year-old female comes to the physician because of fever and worsening cough for the past 4-days. She has had several episodes of otitis media, sinusitis, and an intermittent cough productive of green sputum for the past 2-years. She has also noticed some streaks of blood in the sputum lately. Her temperature is 38°C (100.4°F). Auscultation of the chest reveals crackles and rhonchi bilaterally. Heart sounds cannot be heard along the left lower chest. A CT scan of the chest reveals bronchiectasis and dextrocardia. Which of the following additional findings is most likely in this patient?
A 12-year-old boy presents with progressive clumsiness and difficulty walking. He walks like a 'drunken-man' and has experienced frequent falls. He was born at term and has gone through normal developmental milestones. His vaccination profile is up to date. He denies fever, chills, nausea, vomiting, chest pain, and shortness of breath. He has no history of alcohol use or illicit drug use. His elder brother experienced the same symptoms. The physical examination reveals normal higher mental functions. His extraocular movements are normal. His speech is mildly dysarthric. His muscle tone and strength in all 4 limbs are normal. His ankle reflexes are absent bilaterally with positive Babinski’s signs. Both vibration and proprioception are absent bilaterally. When he is asked to stand with his eyes closed and with both feet close together, he sways from side to side, unable to stand still. X-ray results show mild scoliosis. Electrocardiogram results show widespread T-wave inversions. His fasting blood glucose level is 143 mg/dL. What is the most likely diagnosis?
A 36-year-old woman presents to the emergency department with chest discomfort and fatigue. She reports that her symptoms began approximately 1 week ago and are associated with shortness of breath, swelling of her legs, and worsening weakness. She’s been having transitory fevers for about 1 month and denies having similar symptoms in the past. Medical history is significant for systemic lupus erythematosus (SLE) treated with hydroxychloroquine. She had a SLE flare approximately 2 weeks prior to presentation, requiring a short course of prednisone. Physical exam was significant for a pericardial friction rub. An electrocardiogram showed widespread ST-segment elevation and PR depression. After extensive work-up, she was admitted for further evaluation, treatment, and observation. Approximately 2 days after admission she became unresponsive. Her temperature is 100°F (37.8°C), blood pressure is 75/52 mmHg, pulse is 120/min, and respirations are 22/min. Heart sounds are muffled. Which of the following is a clinical finding that will most likely be found in this patient?
A 54-year-old man presents to the office complaining of recent shortness of breath and fever. He has a history of a chronic cough which is progressively getting worse. His medical history is significant for hypertension and diabetes mellitus, both controlled with medication. He has been working in a sandblasting factory for over 3 decades. His temperature is 37.7°C (99.9°F), the blood pressure is 130/84 mm Hg, the pulse is 98/min, and the respiratory rate is 20/min. Chest X-ray reveals calcified hilar lymph nodes which look like an eggshell. This patient is at increased risk for which of the following conditions?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app