
Cardiology — MCQs

On this page
A 65-year-old man presents to the diabetes clinic for a check-up. He has been successfully managing his diabetes through diet alone, and has not experienced any complications related to retinopathy, neuropathy, or nephropathy. He recently started a new exercise regimen and is eager to see whether his weight has declined since his last visit. The nurse measures his height to be 170 cm and his weight to be 165 lb (75 kg). What range does this patient’s body mass index currently fall into?
A 55-year-old caucasian man presents to his primary care physician with a complaint of double vision, which started suddenly with no precipitating trauma. Twelve years ago, he presented to his physician with painful vision loss, which has since resolved. Since that initial episode, he had numerous episodes early-on in his disease course: two additional episodes of painful vision loss, as well as three episodes of right arm weakness and three episodes of urinary retention requiring catheterization. All of his prior episodes responded to supportive therapy and steroids. Which of the following features of this patient's disease is linked to a more benign disease course?
A 26-year-old man presents to the emergency department complaining of hemoptysis for the past day. He has also experienced fatigue, weight loss (10 kg (22 lb) over the last 2 months), and occasional dry cough. He is a college student and works part-time as a cashier in a bookstore. He is sexually active with his girlfriend and uses condoms occasionally. He smokes 2–3 cigarettes on weekends and denies alcohol use. Today, his pulse is 97/min, the blood pressure is 128/76 mm Hg, the temperature is 36.7°C (98.0°F). On physical exam, the patient is well developed with mild gynecomastia. His heart has a regular rate and rhythm. Lung examination reveals vesicular sounds with occasional crepitations bilaterally. The abdominal exam is non-contributory. His right testicle is tender and larger than the left. The swelling does not transilluminate and does not change in size after performing a Valsalva maneuver. His laboratory work is positive for elevated levels of beta-HCG. What is the most likely diagnosis in this patient?
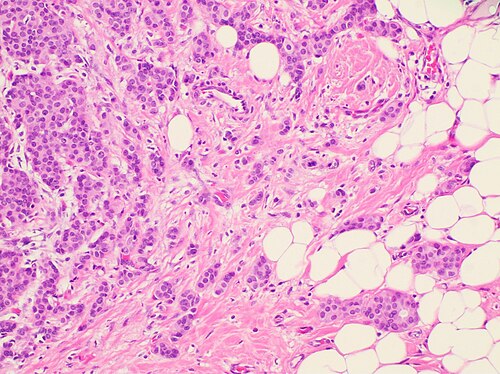
An 80-year-old woman presents with fatigue and a 30-lb weight loss over the past 3 months. The patient states that her symptoms started with mild fatigue about 4 months ago, which have progressively worsened. She noticed that the weight loss started about 1 month later, which has continued despite no changes in diet or activity level. The past medical history is significant for a total abdominal hysterectomy (TAH), and bilateral salpingo-oophorectomy at age 55 for stage 1 endometrial cancer. The patient takes no current medications but remembers taking oral (estrogen/progesterone) contraceptives for many years. The menarche occurred at age 10, and the menopause was at age 50. There is no significant family history. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 120/75 mm Hg, pulse 97/min, respiratory rate 17/min, and oxygen saturation 98% on room air. The physical examination is significant for a palpable mass in the upper outer quadrant of the left breast. The mass is hard and fixed with associated axillary lymphadenopathy. The mammography of the left breast shows a spiculated mass in the upper outer quadrant. An excisional biopsy of the mass is performed, and the histologic examination reveals the following significant findings (see image). Immunohistochemistry reveals that the cells from the biopsy are estrogen receptor (ER)/progesterone receptor (PR) and human epidermal growth factor receptor-2 (HER-2)/neu positive. Which of the following is the most important indicator of a poor prognosis for this patient?
A 46-year-old woman comes to the physician with a 4-month history of lethargy. She has had joint pain for the past 15 years and does not have a primary care physician. Her temperature is 37.4°C (99.3°F), pulse is 97/min, and blood pressure is 132/86 mm Hg. Physical examination shows pallor of the oral mucosa and nontender subcutaneous nodules on both elbows. The distal interphalangeal joints of both hands are flexed and the proximal interphalangeal joints appear hyperextended. Range of motion in the fingers is restricted. The liver span is 6 cm and the spleen tip is palpated 4 cm below the left costal margin. Laboratory studies show: Hematocrit 33% Leukocyte count 1,800/mm3 Segmented neutrophils 35% Lymphocytes 60% Platelet count 130,000/mm3 Increased serum titers of which of the following is most specific for this patient's condition?
An 85-year-old man presents to his primary care provider after feeling "lightheaded." He said he helped his wife in the garden for the first time, but that while moving some bags of soil he felt like he was going to faint. He had a big breakfast of oatmeal and eggs prior to working in the garden. He has no significant past medical history and takes a baby aspirin daily. Physical exam reveals an elderly, well-nourished, well-built man with no evidence of cyanosis or tachypnea. Vital signs show normal temperature, BP 150/70, HR 80, RR 18. Cardiac exam reveals crescendo-decrescendo systolic murmur. What is the most likely cause of this patient's diagnosis?
A 33-year-old man is brought into the emergency department with fever, lethargy, and confusion. He is a cachectic man in acute distress, unable to respond to questions or follow commands. His friend confides that the patient has been sexually active with multiple male partners and was diagnosed with HIV several months ago, but was lost to follow up. Based on prior records, his most recent CD4 count was 65 cells/uL. Which of the following is the most appropriate next step in management?
A 40-year-old woman visits her physician’s office with her husband. Her husband says that she has been complaining of recurring headaches over the past few months. A year ago she was diagnosed with diabetes and is currently on treatment for it. About 6 months ago, she was diagnosed with high blood pressure and is also taking medication for it. Her husband is concerned about the short span during which she has been getting all these symptoms. He also says that she occasionally complains of changes and blurring in her vision. In addition to all these complaints, he has observed changes in her appearance, more prominently her face. Her forehead and chin seem to be protruding more than usual. Suspecting a hormonal imbalance, which of the following initial tests would the physician order to indicate a possible diagnosis?
A 62-year-old woman with hypertension and type 2 diabetes mellitus comes to the physician because of increasing shortness of breath and a dry cough over the past 6 months. She has smoked 1 pack of cigarettes daily for the past 40 years. Chest auscultation shows scattered expiratory wheezes in both lung fields. Spirometry shows an FEV1:FVC ratio of 65% and an FEV1 of 70% of predicted. Her diffusing capacity for carbon monoxide (DLCO) is 42% of predicted. Which of the following is the most likely diagnosis?
A 55-year-old male smoker presents to your office with hemoptysis, central obesity, and a round face with a "moon-like" appearance. He is found to have a neoplasm near the hilum of his left lung. A biopsy of the tumor reveals small basophilic cells with finely granular nuclear chromatin (a "salt and pepper" pattern). Which of the following is the most appropriate treatment for this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app