
Cardiology — MCQs

On this page
A 52 year-old woman comes to the physician because of intense retrosternal chest pain for the last three days. The pain is worse with breathing or coughing, and improves while sitting upright. She also reports a mild fever and shortness of breath. She was diagnosed with chronic kidney disease secondary to lupus nephritis 12 years ago and has been on hemodialysis since then, but she missed her last two appointments because of international travel. She also underwent a percutaneous coronary intervention eight months ago for a myocardial infarction. She takes azathioprine after hemodialysis. Her temperature is 37.8°C (100°F), pulse is 110/min, and blood pressure is 130/84 mm Hg. The lungs are clear to auscultation bilaterally with normal breath sounds. Cardiac examination reveals a high-pitched scratching that obscures both heart sounds. The remainder of the examination is otherwise unremarkable. Cardiac enzyme levels and anti-DNA antibodies are within normal limits. An x-ray of the chest shows no abnormalities. An ECG shows Q waves in the anterior leads. Which of the following is the most likely cause of these findings?
A 72-year-old man is brought to the physician by his wife for forgetfulness, confusion, and mood changes for the past 4 months. His symptoms started with misplacing items such as his wallet and keys around the house. Two months ago, he became unable to manage their finances as it became too difficult for him. Last week, he became lost while returning home from the grocery store. His wife reports that he shows “no emotion” and that he is seemingly not concerned by his recent symptoms. He has hypertension, type 2 diabetes mellitus, and coronary artery disease. Current medications include aspirin, metoprolol, lisinopril, metformin, and rosuvastatin. His pulse is 56/min and blood pressure is 158/76 mm Hg. Neurologic examination shows loss of sensation on his right leg and an unsteady gait. When asked to stand with his eyes closed and palms facing upward, his right arm rotates inward. An MRI of the brain shows multiple deep white matter lesions. Which of the following is the most likely diagnosis?
A 76-year-old woman presents to her primary care physician with an intense, throbbing, right-sided headache. She has a history of migraine headaches and tried her usual medications this afternoon with no alleviation of symptoms. She states that this headache feels different because she also has pain in her jaw that is worse with chewing. The pain came on gradually and is getting worse. In addition, over the past few months, she has had some difficulty getting up out of chairs and raising both her arms over her head to put on her clothes. She has had no recent falls or injuries. On exam, the patient's temperature is 98.3°F (36.8°C), blood pressure is 115/70 mmHg, pulse is 93/min, and respirations are 15/min. The patient has tenderness over her right temple. She has no focal neurological deficits, and no abnormalities on fundoscopic exam. Her physical exam is otherwise within normal limits. Given the patient's most likely diagnosis, which of the following methods of treatment should be used in order to prevent any further complications?
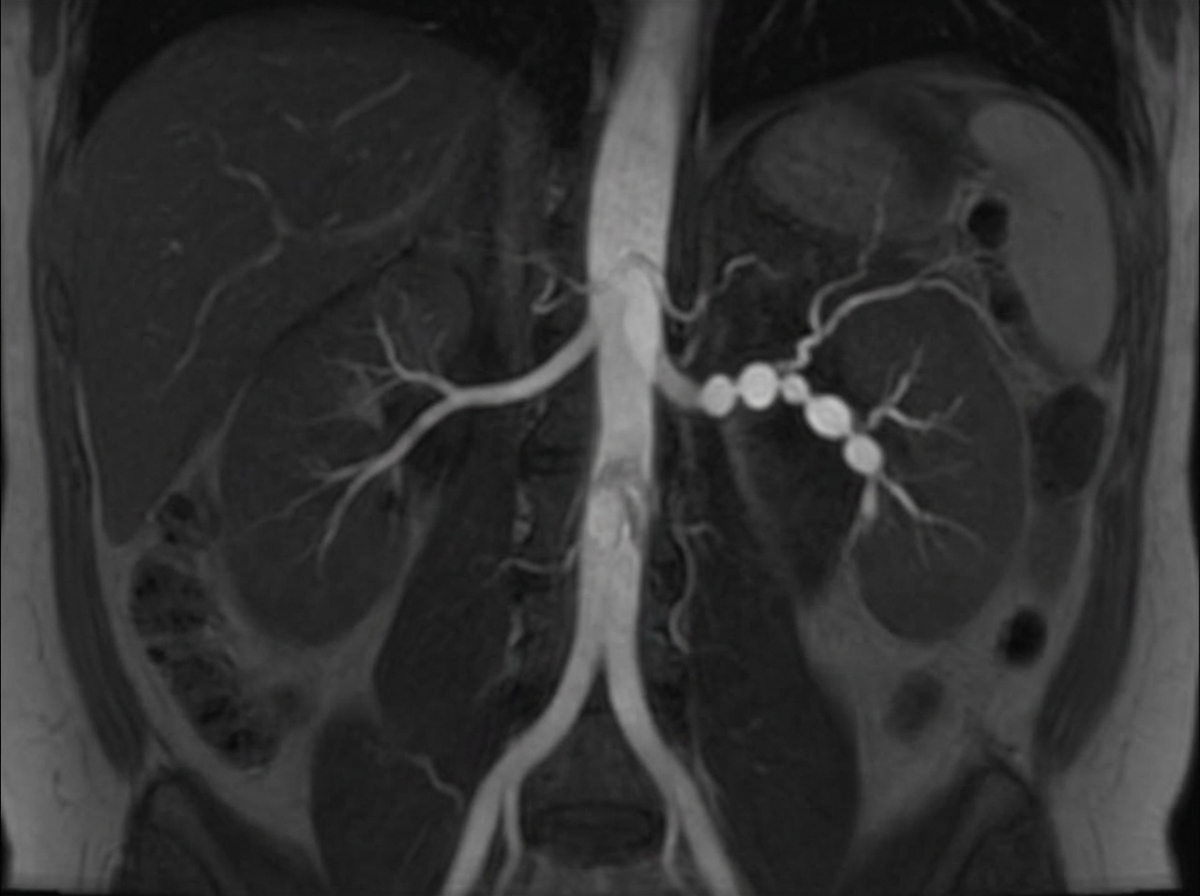
A 31-year-old woman returns to her primary care provider for a follow-up visit. At a routine health maintenance visit 2 months ago, her blood pressure (BP) was 181/97 mm Hg. She has adhered to a low-salt diet and exercises regularly. On repeat examination 1 month later, her BP was 178/93, and she was prescribed hydrochlorothiazide and lisinopril. The patient denies any complaint, except for occasional headaches. Now, her BP is 179/95 in the right arm and 181/93 in the left arm. Physical examination reveals an abdominal bruit that lateralizes to the left. A magnetic resonance angiogram of the renal arteries is shown in the image. Which of the following is the best next step for the management of this patient condition?
A 32-year-old woman presents with progressive shortness of breath and a dry cough. She says that her symptoms onset recently after a 12-hour flight. Past medical history is unremarkable. Current medications are oral estrogen/progesterone containing contraceptive pills. Her vital signs include: blood pressure 110/60 mm Hg, pulse 101/min, respiratory rate 22/min, oxygen saturation 88% on room air, and temperature 37.9℃ (100.2℉). Her weight is 94 kg (207.2 lb) and height is 170 cm (5 ft 7 in). On physical examination, she is acrocyanotic. There are significant swelling and warmth over the right calf. There are widespread bilateral rales present. Cardiac auscultation reveals accentuation of the pulmonic component of the second heart sound (P2) and an S3 gallop. Which of the following ventilation/perfusion (V/Q) ratios most likely corresponds to this patient’s condition?
A 43-year-old man with HIV comes to the physician because of fever and night sweats over the past 15 days. During this period, he has also had headaches and generalized weakness. He has no cough or shortness of breath. He has hypertension controlled with lisinopril and is currently receiving triple antiretroviral therapy. He has smoked one pack of cigarettes daily for the past 15 years and drinks one to two beers on weekends. He is a known user of intravenous illicit drugs. His temperature is 39°C (102°F), pulse is 115/min, respirations are 15/min, and blood pressure is 130/80 mm Hg. Examination shows several track marks on the forearms. The lungs are clear to auscultation. A holosystolic murmur that increases on inspiration is heard along the left sternal border. The remainder of the physical examination shows no abnormalities. Laboratory studies show a leukocyte count of 12,800/mm3 and an erythrocyte sedimentation rate of 52 mm/h. His CD4+ T-lymphocyte count is 450/mm3 (normal ≥ 500). Which of the following is the most likely sequela of the condition?
A 50-year-old man presents to the emergency department with a severe headache. The patient reports that it started approx. 2 hours ago and has steadily worsened. He describes it as a stabbing pain localized behind his left eye. The patient reports that he has been having similar headaches several times a day for the past week, most often at night. He denies any nausea, vomiting, and visual or auditory disturbances. He has no significant past medical history. Current medications are a multivitamin and caffeine pills. The patient reports regular daily alcohol use but does not smoke. His temperature is 37.0°C (98.6°F), the blood pressure is 120/70 mm Hg, the pulse is 85/min, the respiratory rate is 18/min, and the oxygen saturation is 99% on room air. The patient is in moderate distress from the pain. The physical exam is significant for unilateral diaphoresis on the left forehead, left-sided rhinorrhea, and pronounced lacrimation of the left eye. The remainder of the physical exam is normal. Laboratory tests are normal. Non-contrast CT of the head shows no evidence of intracranial masses or hemorrhage. High flow oxygen and fluid resuscitation are initiated. Ibuprofen 200 mg orally is administered. Despite these interventions, the patient continues to be in significant pain. What is the next best step in management?
A 77-year-old woman is brought by ambulance to the emergency department after she developed weakness of her right arm along with a right-sided facial droop. By the time the ambulance arrived, she was having difficulty speaking. Past medical history is significant for hypertension, diabetes mellitus type II, and hyperlipidemia. She takes lisinopril, hydrochlorothiazide, metformin, and atorvastatin. On arrival to the emergency department, her vital signs are within normal limits. On physical examination, she is awake and alert but the right side of her mouth is dropping, making it difficult for her to speak clearly. Her heart has a regular rate and rhythm and her lungs are clear to auscultation bilaterally. Fingerstick glucose is 85 mg/dL. Her right upper extremity strength is 2/5 and her left upper extremity strength is 5/5. Which of the following is the best next step in management?
A 44-year-old man is brought to the emergency department after sustaining high-voltage electrical burns over his left upper limb. On examination, the tip of his left middle finger is charred, and there are 2nd-degree burns involving the whole of the left upper limb. Radial and ulnar pulses are strong, and there are no signs of compartment syndrome. An exit wound is present over the sole of his right foot. His temperature is 37.7°C (99.8°F), the blood pressure is 110/70 mm Hg, the pulse is 105/min, and the respiratory rate is 26/min. His urine is reddish-brown, and urine output is 0.3 mL/kg/h. Laboratory studies show: Hemoglobin 13.9 g/dL Hematocrit 33% Leukocyte count 11,111/mm3 Serum Creatinine 4.6 mg/dL Creatine phosphokinase 15,230 U/L K+ 7.7 mEq/L Na+ 143 mEq/L What is the most likely mechanism for this patient's renal failure?
A 34-year-old primigravida presents with progressive shortness of breath on exertion and while sleeping. The patient says that she uses 2 pillows to breathe comfortably while sleeping at night. These symptoms started in the 3rd week of the 2nd trimester of pregnancy. She does not have any chronic health problems. She denies smoking and alcohol intake. Vital signs include: blood pressure 110/50 mm Hg, temperature 36.9°C (98.4°F), and regular pulse 90/min. Previous physical examination in the 1st trimester had disclosed no cardiac abnormalities, but on current physical examination, she has a loud S1 and a 2/6 diastolic rumble over the cardiac apex. A transthoracic echocardiogram shows evidence of mitral valve stenosis. Which of the following is the best initial treatment for this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app