
Cardiology — MCQs

On this page
A 33-year-old woman presents to the physician because of abdominal discomfort, weakness, and fever. She has had a significant weight loss of 15 kg (33.1 lb) over the past 2 months. She has no history of medical illness and is not on any medications. Her pulse is 96/min, the blood pressure is 167/92 mm Hg, the respiratory rate is 20/min, and the temperature is 37.7°C (99.8°F). Her weight is 67 kg (147.71 lb), height is 160 cm (5 ft 3 in), and BMI is 26.17 kg/m2. Abdominal examination shows purple striae and a vaguely palpable mass in the left upper quadrant of the abdomen, which does not move with respirations. She has coarse facial hair and a buffalo hump along with central obesity. Her extremities have poor muscle bulk, and muscle weakness is noted on examination. An ultrasound of the abdomen demonstrates an adrenal mass with para-aortic lymphadenopathy. Which of the following is the most likely laboratory profile in this patient?
A 27-year-old Caucasian female presents to her physician for episodes of urinary incontinence that began shortly after a breakup with her boyfriend. She claimed to be psychologically devastated when she found him sleeping with her brother and has had trouble caring for herself ever since. The patient states that the episodes came on suddenly and occur randomly. The patient denies any burning or pain upon urination. Upon obtaining further history, the patient also states that she has "stress spells" in which her vision becomes blurry or has blind spots. The patient also complains of frequent headaches. These symptoms have persisted for the past few years and she attributes them to arguments with her boyfriend. Embarrassed, the patient even admits to episodes of fecal incontinence which she also blames on her boyfriend's perpetual verbal and occasional physical abuse. The patient is teary and a physical exam is deferred until her mood improves. Which of the following is the most appropriate next step in management?
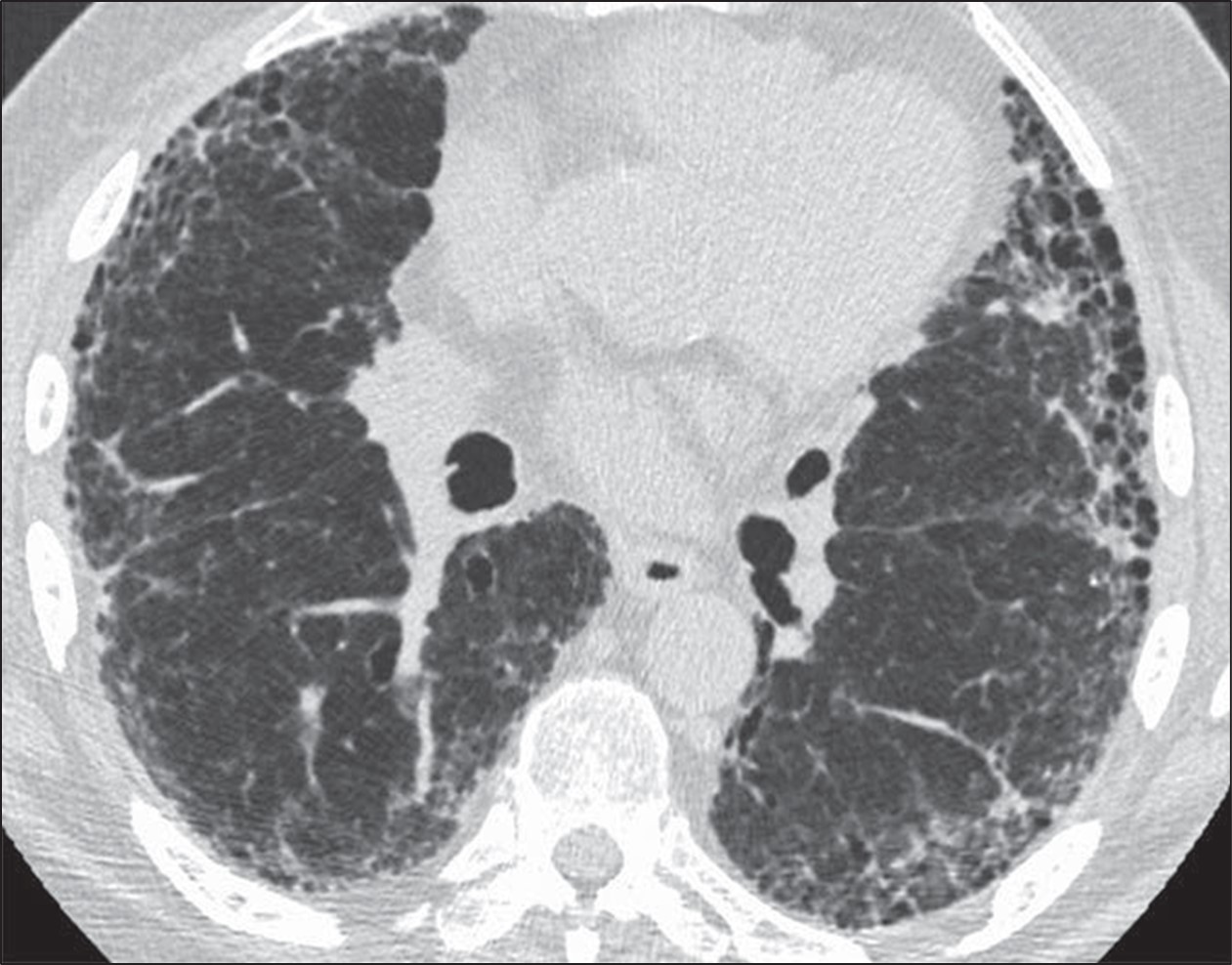
A 52-year-old man comes to the physician because of a 6-month history of shortness of breath and nonproductive cough. He has smoked 1 pack of cigarettes daily for 15 years. Cardiopulmonary examination shows fine inspiratory crackles bilaterally. There is clubbing present in the fingers bilaterally. Pulmonary function tests (PFTs) show an FVC of 78% of expected and an FEV1/FVC ratio of 92%. A CT scan of the chest is shown. Which of the following is the most likely underlying diagnosis?
A 24-year-old man presents with a complaint of breathlessness while jogging. He says that he recently started marathon training. He does not have any family history of asthma nor has any allergies. He currently takes no medication. The blood pressure is 120/80 mm Hg, and the heart rate is 67/min. With each heartbeat, he experiences pounding in his chest, and his head bobs. On physical examination, he has long fingers, funnel chest, and disproportionate body proportions with a decreased upper-to-lower segment ratio. On auscultation over the 2nd right intercostal space, an early diastolic murmur is heard, and 3rd and 4th heart sounds are heard. Echocardiography shows aortic root dilatation. The patient is scheduled for surgery. Which of the following is associated with this patient's condition?
A 38-year-old woman comes to the physician because of frequent headaches and blurring of vision. She also complains of weight gain, menstrual irregularities, and excessive growth of body hair. She says that, for the first time since she turned 18, her shoe and ring sizes have increased, and also complains that her voice has become hoarser. She does not smoke or drink alcohol. She takes no medications. Vital signs are within normal limits. Physical examination shows prominent frontal bossing, a protuberant mandible with spaces between the teeth, and large hands and feet. Serum studies show: Na+ 140 mEq/L Cl− 102 mEq/L K+ 4.1 mEq/L Ca2+ 10.6 mg/dL Phosphorus 4.7 mg/dL Glucose 180 mg/dL Which of the following is the most likely sequela of this patient's condition?
A 47-year-old man comes to the physician for a routine health maintenance examination. He has no complaints and has no history of serious illness. He works as a forklift operator in a factory. His brother died of malignant melanoma. He smokes occasionally and drinks a glass of wine once a week. His pulse is 79/min and blood pressure is 129/84 mm Hg. Which of the following causes of death is this patient most at risk for over the next 15 years?
A 62-year-old man comes to the physician because of fatigue and swelling of the lower legs for 3 weeks. One year ago, he had an 85% stenosis in the left anterior descending artery, for which he received 2 stents. He was diagnosed with hepatitis C 5 years ago. He has type 2 diabetes mellitus and arterial hypertension. Current medications include aspirin, metformin, and ramipril. He does not smoke or drink alcohol. His temperature is 37°C (98.6°F), pulse is 92/min, and blood pressure is 142/95 mm Hg. Examination shows 2+ pretibial edema bilaterally. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 10.2 g/dL Leukocyte count 6500/mm3 Platelet count 188,000/mm3 Serum Na+ 137 mEq/L Cl− 105 mEq/L K+ 5.2 mEq/L Urea nitrogen 60 mg/dL Glucose 110 mg/dL Creatinine 3.9 mg/dL Albumin 3.6 g/dL HbA1C 6.8% Urine Blood negative Glucose 1+ Protein 3+ WBC 0–1/hpf A renal biopsy shows sclerosis in the capillary tufts and arterial hyalinosis. Which of the following is the most likely underlying mechanism of this patient's findings?
A tall, slender 32-year-old man comes to the emergency room because of sudden chest pain, cough, and shortness of breath. On physical examination, he has decreased breath sounds on the right. Chest radiography shows translucency on the right side of his chest. His pCO2 is elevated and pO2 is decreased. What is the most likely cause of his symptoms?
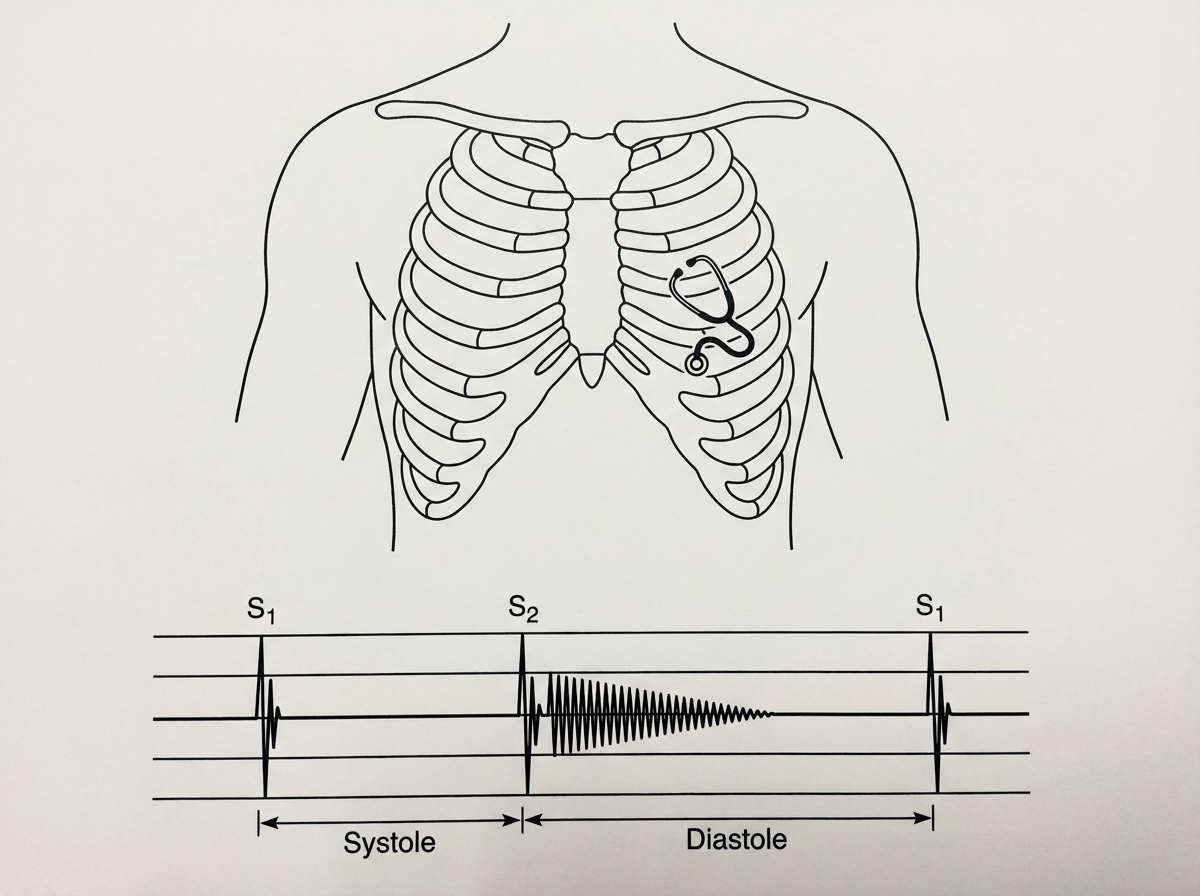
An otherwise healthy 25-year-old man comes to the physician because of a 3-month history of intermittent palpitations and worsening shortness of breath on exertion. He has not had chest pain or nocturnal dyspnea. The patient is 195 cm (6 ft 5 in) tall and weighs 70 kg (154 lbs); BMI is 18.4 kg/m2. His pulse is 110/min and blood pressure is 140/60 mm Hg. The lungs are clear to auscultation. Cardiac examination is shown. Which of the following is the most likely diagnosis?
A 25-year-old woman presents to the emergency department with sudden onset of lower limb weakness for the past 2 days. She says she also hasn’t been able to urinate for that same period. There is no history of trauma, fever, weight loss, recent respiratory tract infection, or diarrhea. She has a past medical history of left arm weakness 18 months ago that resolved spontaneously. Her father had type 2 diabetes mellitus, ischemic heart disease, and left-sided residual weakness secondary to an ischemic stroke involving the right middle cerebral artery. Her vital signs include: blood pressure 120/89 mm Hg, temperature 36.7°C (98.0°F), pulse 78/min, and respiration rate 16/min. Muscle strength is 3/5 in both lower limbs with increased tone and exaggerated deep tendon reflexes. The sensation is decreased up to the level of the umbilicus. Muscle strength, tone, and deep tendon reflexes in the upper limbs are normal. On flexion of the neck, the patient experiences electric shock-like sensations that travel down to the spine. Funduscopic examination reveals mildly swollen optic discs bilaterally. Which of the following is the next best step in management for this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app