
Cardiology — MCQs

On this page
A 55-year-old woman comes to the physician because of a 4-day history of chest pain and cough with rust-colored sputum. The chest pain is sharp, stabbing, and exacerbated by coughing. Ten days ago, she had a sore throat and a runny nose. She was diagnosed with multiple sclerosis at the age of 40 years and uses a wheelchair for mobility. She has smoked a pack of cigarettes daily for the past 40 years. She does not drink alcohol. Current medications include ocrelizumab and dantrolene. Her temperature is 37.9°C (100.2°F), blood pressure is 110/60 mm Hg, and pulse is 105/min. A few scattered inspiratory crackles are heard in the right lower lung. Cardiac examination shows no abnormalities. Neurologic examination shows stiffness and decreased sensation of the lower extremities; there is diffuse hyperreflexia. An x-ray of the chest is shown. Which of the following is the most likely cause of her current symptoms?

A 9-year-old girl is brought to the physician by her mother because of a 3-day history of face and foot swelling, dark urine, and a rash on her hands and feet. The mother reports that her daughter has had a low-grade fever, shortness of breath, and a dry cough for the past 8 days. She has had generalized weakness and pain in her right knee and ankle. She has a ventricular septum defect that was diagnosed at birth. The patient appears lethargic. Her temperature is 38.4 (101.1°F), pulse is 130/min, respirations are 34/min, and blood pressure is 110/60 mm Hg. Examination shows small, non-blanching, purple lesions on her palms, soles, and under her fingernails. There is edema of the eyelids and feet. Funduscopic examination shows retinal hemorrhages. Holosystolic and early diastolic murmurs are heard. Laboratory studies show: Hemoglobin 11.3 g/dL Erythrocyte sedimentation rate 61 mm/h Leukocyte count 15,000/mm3 Platelet count 326,000/mm3 Urine Blood 4+ Glucose negative Protein 1+ Ketones negative Transthoracic echocardiography shows a small outlet ventricular septum defect and a mild right ventricular enlargement. There are no wall motion abnormalities, valvular heart disease, or deficits in the pump function of the heart. Blood cultures grow Streptococcus pyogenes. Which of the following is the most likely diagnosis?
A 65-year-old woman comes to the physician because of increased difficulty hearing. She has also had dull and progressive pain in her hip and lower back for the past 2 months that is worse with exertion. Examination of the ears shows impaired hearing on the left with whispered voice test and lateralization to the right with Weber testing. There is localized tenderness over the right hip and groin area with decreased range of motion of the hip. The remainder of the examination shows no abnormalities. Serum studies show: Total protein 6.5 g/dL Alkaline phosphatase 950 U/L Calcium 9 mg/dL Phosphorus 4 mg/dL Which of the following is the most likely underlying mechanism of this patient's symptoms?
A 57-year-old man presents to his primary care provider because of chest pain for the past 3 weeks. The chest pain occurs after climbing more than 2 flight of stairs or walking for more than 10 minutes and resolves with rest. He is obese, has a history of type 2 diabetes mellitus, and has smoked 15-20 cigarettes a day for the past 25 years. His father died from a myocardial infarction at 52 years of age. Vital signs reveal a temperature of 36.7 °C (98.06°F), a blood pressure of 145/93 mm Hg, and a heart rate of 85/min. The physical examination is unremarkable. Which of the following best represents the most likely etiology of the patient’s condition?
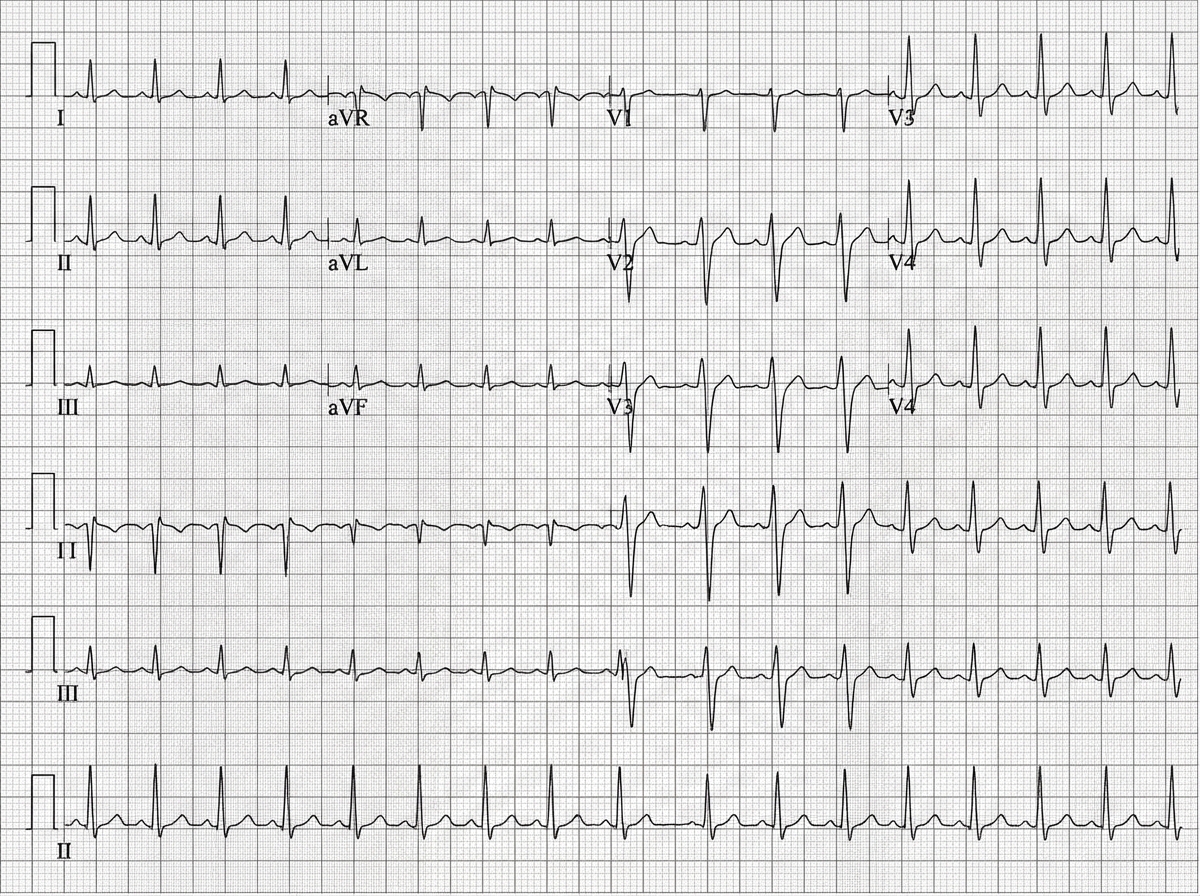
A 45-year-old man is brought to the emergency department after a car accident with pain in the middle of his chest and some shortness of breath. He has sustained injuries to his right arm and leg. He did not lose consciousness. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 18/min, and blood pressure is 90/60 mm Hg. He is alert and oriented to person, place, and time. Examination shows several injuries to the upper extremities and chest. There are jugular venous pulsations 10 cm above the sternal angle. Heart sounds are faint on cardiac examination. The lungs are clear to auscultation. An ECG is shown. Which of the following is the most appropriate next step in management?
A 48-year-old man comes to the emergency department because of sudden right flank pain that began 3 hours ago. He also noticed blood in his urine. Over the past two weeks, he has developed progressive lower extremity swelling and a 4-kg (9-lb) weight gain. Examination shows bilateral 2+ pitting edema of the lower extremities. Urinalysis with dipstick shows 4+ protein, positive glucose, and multiple red cell and fatty casts. Abdominal CT shows a large right kidney with abundant collateral vessels and a filling defect in the right renal vein. Which of the following is the most likely underlying cause of this patient's symptoms?
A 67-year-old male with a history of poorly controlled hypertension, COPD, and diabetes presents to his cardiologist for a routine appointment. He reports that he has no current complaints and has not noticed any significant changes in his health. On exam, the cardiologist hears an extra heart sound in late diastole that immediately precedes S1. This heart sound is most associated with which of the following?
A 54-year-old man is brought to the emergency department 1 hour after an episode of loss of consciousness that lasted 3 minutes. Since awakening, he has had weakness of the left arm and leg, and his speech has been slurred. He has had a fever for 10 days. He has not had vomiting or headache. He was treated for bacterial sinusitis 3 weeks ago with amoxicillin-clavulanate. He has hypertension, hypothyroidism, hyperlipidemia, and type 2 diabetes mellitus. Current medications include amlodipine, hydrochlorothiazide, metformin, simvastatin, aspirin, and levothyroxine. His temperature is 38.6°C (101.4°F), pulse is 106/min, and blood pressure is 160/90 mm Hg. He is alert and oriented to person, place, and time. Examination shows multiple petechiae on his trunk and painless macules over both palms. A new grade 3/6 systolic murmur is heard best at the apex. He follows commands, but he slurs his words and has difficulty naming common objects. There is left facial droop. Muscle strength is 4/5 in the left upper and lower extremities. Deep tendon reflexes are 3+ on the left side and 2+ on the right side. The left big toe shows an extensor response. Fundoscopic examination shows retinal hemorrhages with white centers. Laboratory studies show: Hemoglobin 15.3 g/dL Leukocyte count 12,300/mm3 Serum Na+ 136 mEq/L Cl- 103 mEq/L K+ 4.3 mEq/L Glucose 108 mg/dL Creatinine 1.1 mg/dL Urine Protein 1+ Glucose negative Blood 1+ WBC 1–2/hpf RBC 7–10/hpf Which of the following is the most likely cause of these findings?
A 34-year-old woman, who had her first child 2 weeks ago, visits her family physician with concerns about constant fatigue and difficulty with breastfeeding. She was discharged from the intensive care unit after hospitalization for severe postpartum hemorrhage. Since then, she has tried multiple pumps and self-stimulation to encourage breast milk production; however, neither of these strategies has worked. Her blood pressure is 88/56 mm Hg and heart rate is 120/min. Which of the following best explains the underlying condition of this patient?
A 58-year-old woman is brought to the emergency department because of a 2-day history of increasing chest pain and shortness of breath. She has had a productive cough with foul-smelling sputum for 1 week. Seven months ago, the patient had an ischemic stroke. She has gastritis and untreated hypertension. She currently lives in an assisted-living community. She has smoked one pack of cigarettes daily for 40 years. She has a 20-year history of alcohol abuse, but has not consumed any alcohol in the past 4 years. Her only medication is omeprazole. She appears to be in respiratory distress and speaks incoherently. Her temperature is 39.3°C (102.7°F), pulse is 123/min, respirations are 33/min, and blood pressure is 155/94 mm Hg. Auscultation of the lung shows rales and decreased breath sounds over the right upper lung field. Examination shows weakness and decreased sensation of the right upper and lower extremities. Babinski sign and facial drooping are present on the right. Arterial blood gas analysis on room air shows: pH 7.48 PCO2 31 mm Hg PO2 58 mm Hg O2 saturation 74% A chest x-ray shows infiltrates in the right posterior upper lobe. Which of the following is the strongest predisposing factor for this patient's respiratory symptoms?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app