
Cardiology — MCQs

On this page
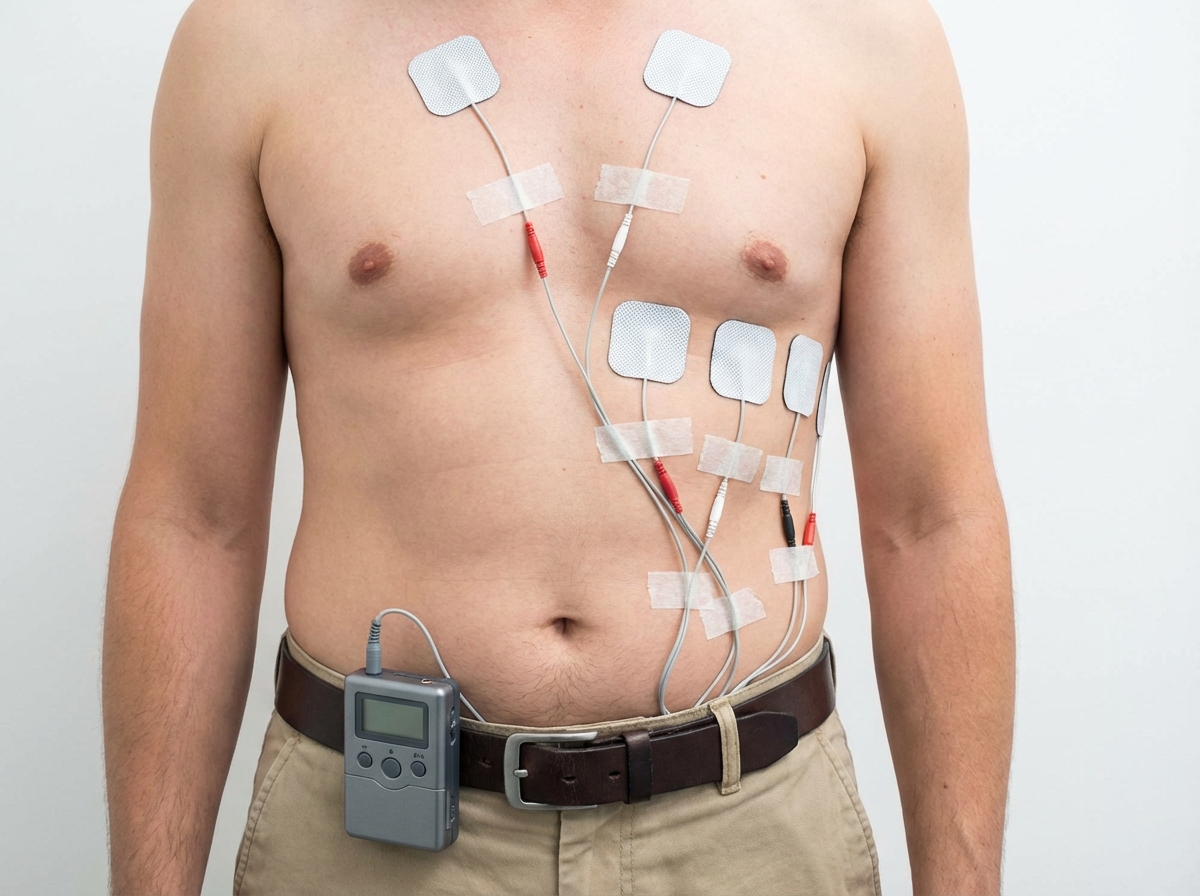
Which score is calculated during performance of this test?

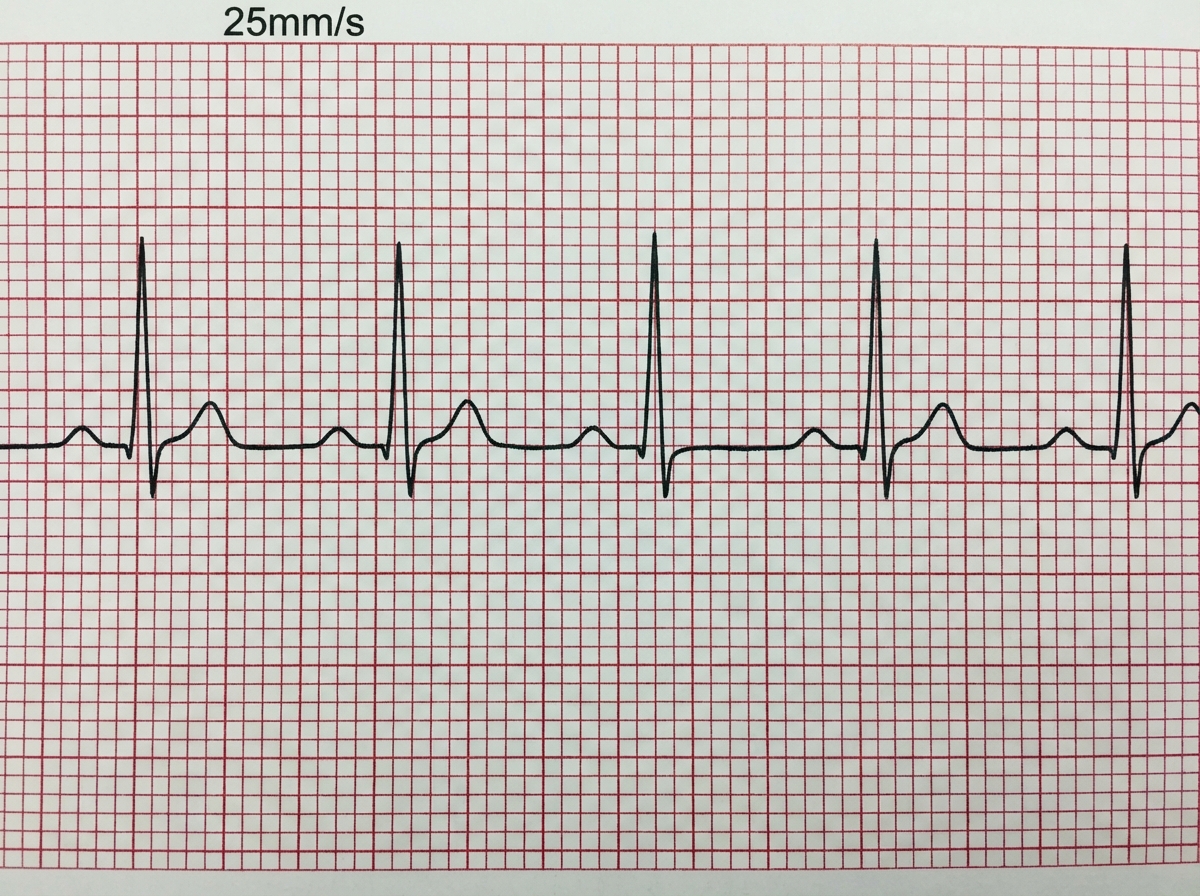
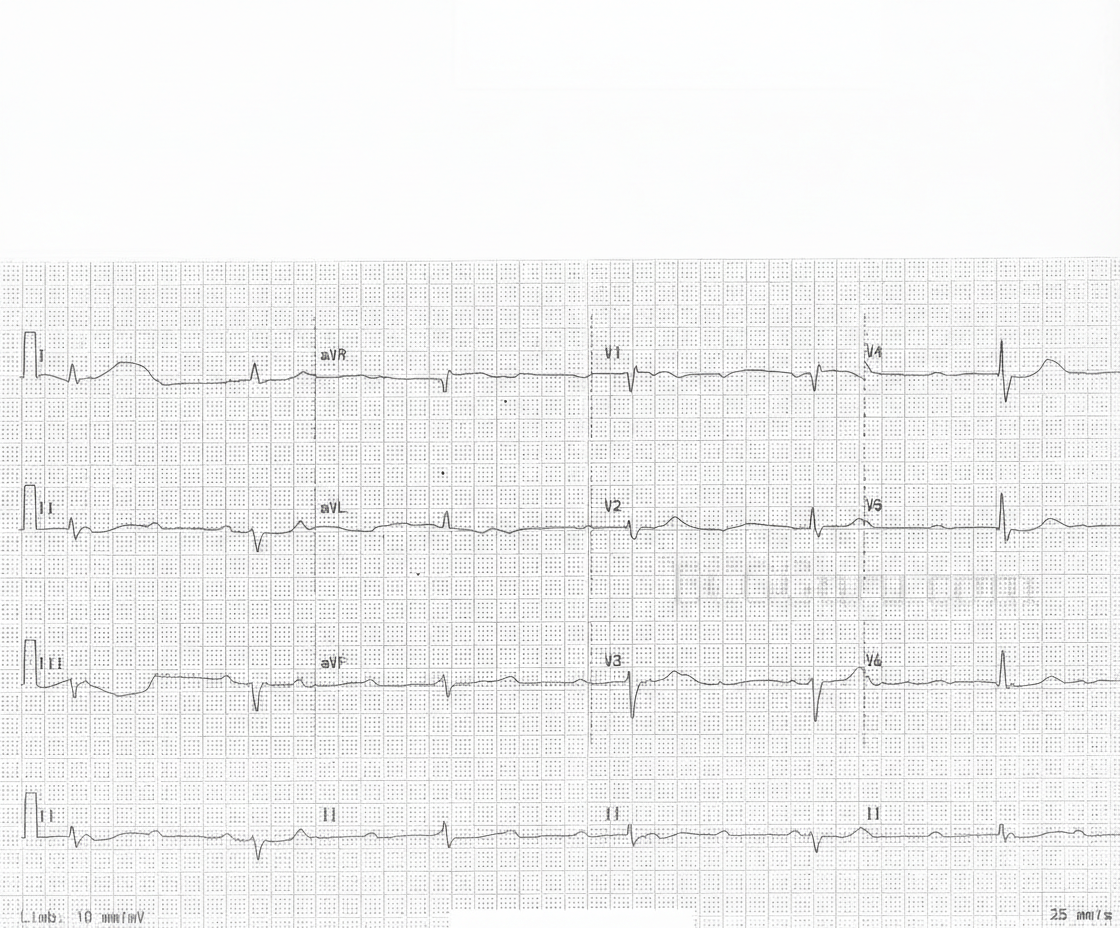
Which is correct about the ECG shown below?
What is not recommended while wearing this cardiac device?

Which device is shown here?
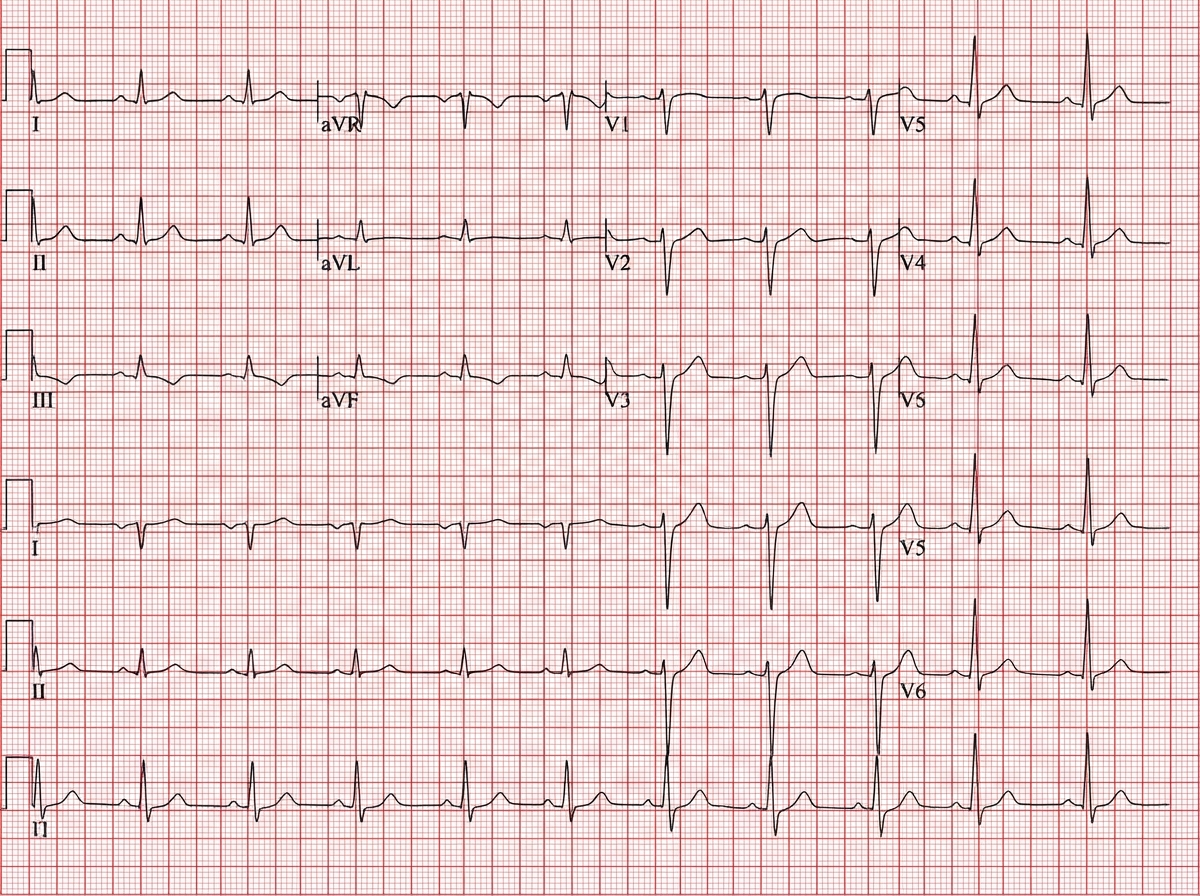
Which of the following describes the marked ECG finding?
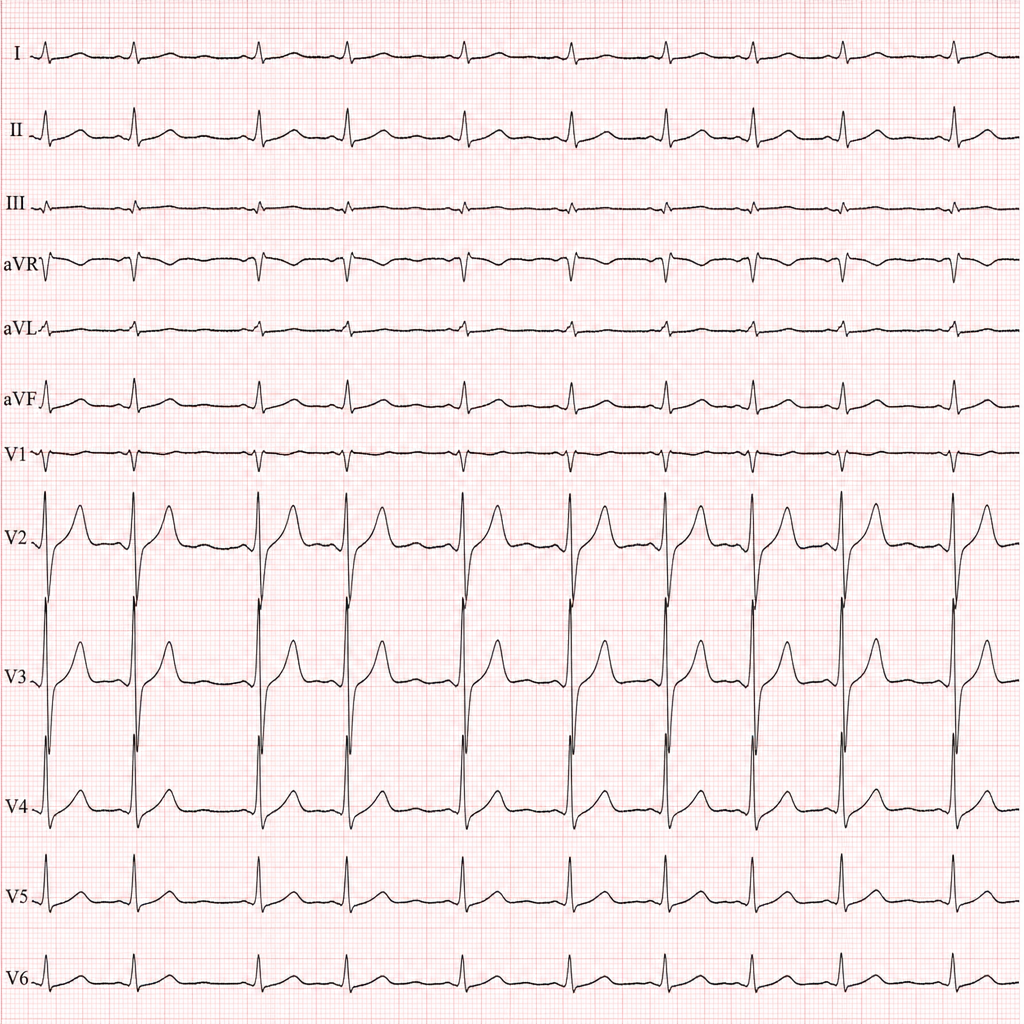
A patient complains of exertional syncope. He gives history of sudden death of his elder brother during a football game. Which of the following ECG findings is seen here?
An 80-year-old woman has had several episodes of dizziness and recently fell, sustaining a hip fracture. The ECG shown demonstrates complete (third-degree) AV block with marked bradycardia. She is hemodynamically stable, and evaluation reveals no reversible cause such as medication toxicity, electrolyte disturbance, or acute myocardial ischemia. What is the next best step in management?
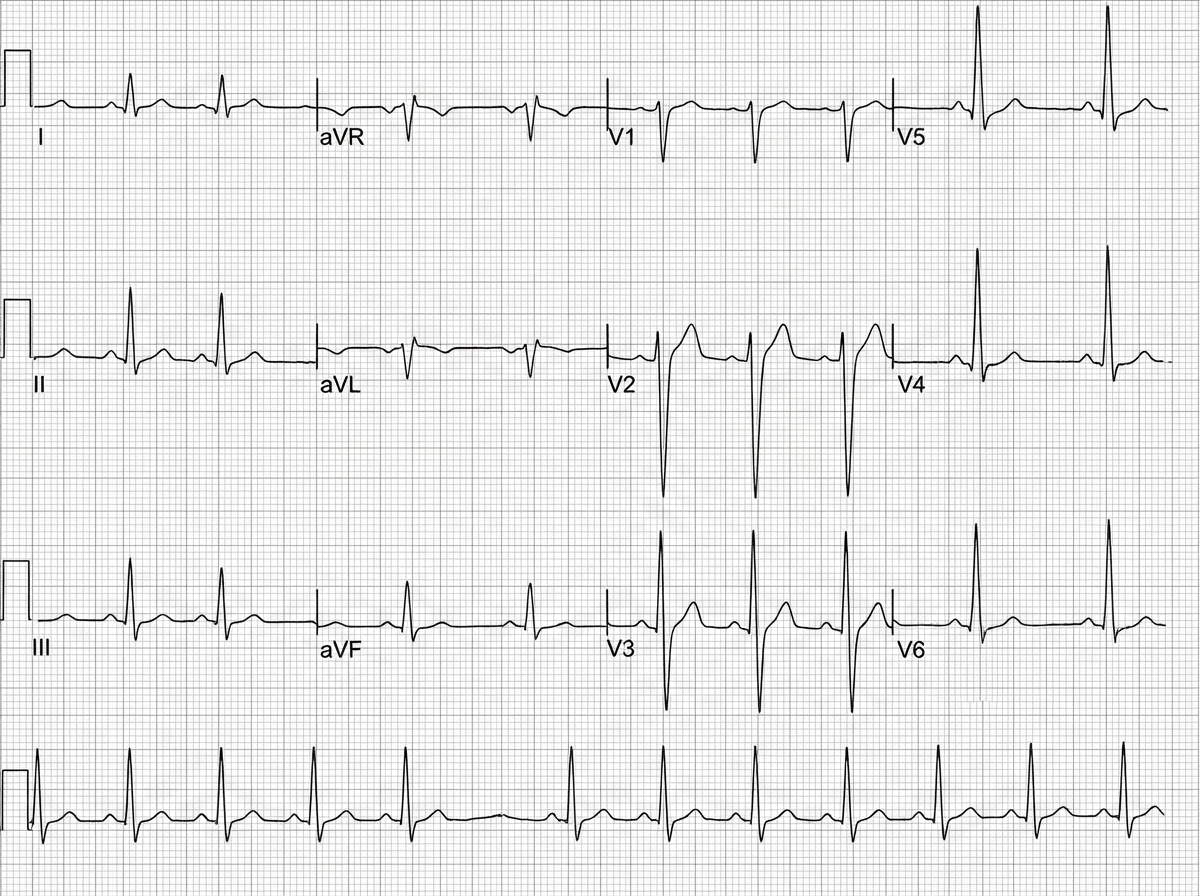
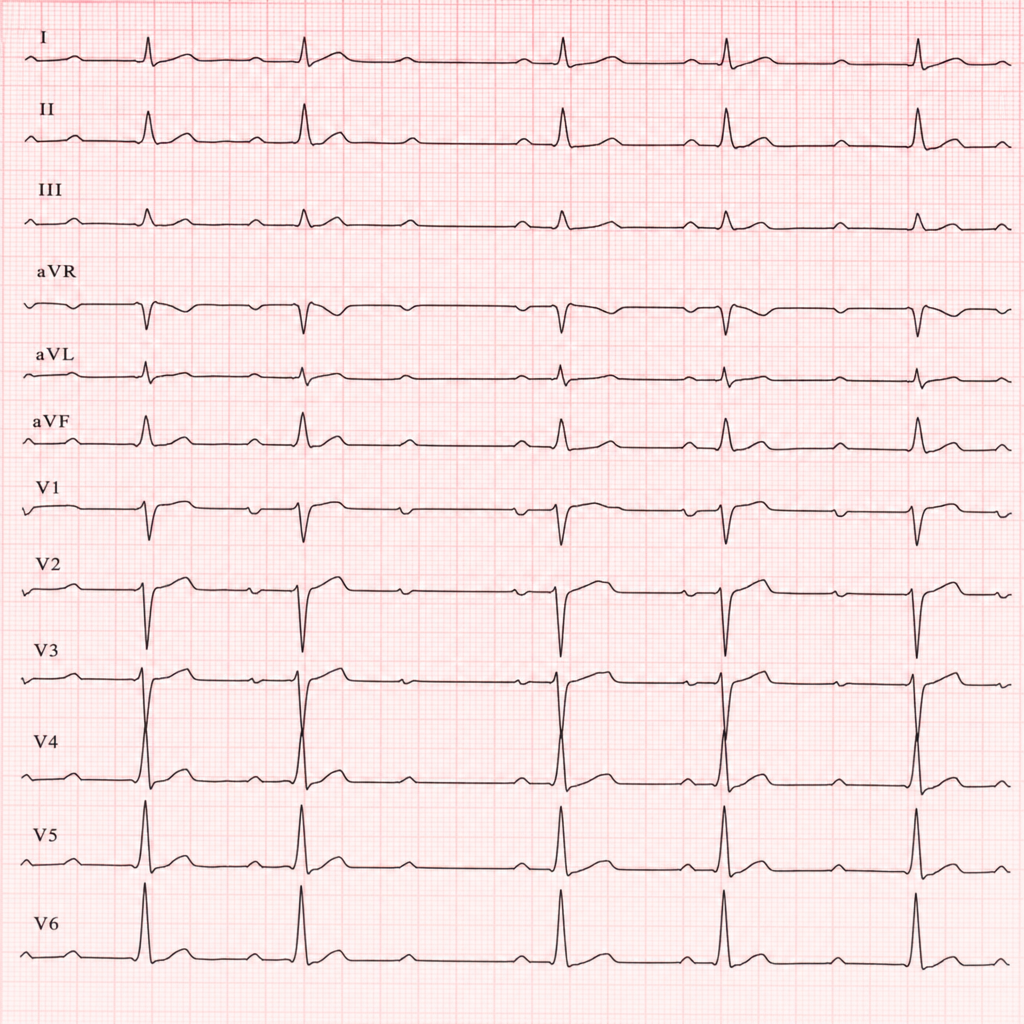
Comment on the diagnosis of the ECG tracing shown below:
A 16-year-old boy presents with recurrent episodes of light headedness followed by syncope in school assembly. ECG was done on arrival to hospital. What is the diagnosis?
274. A young athlete was found to have hypertrophic cardiomyopathy during testing for a competitive sport. Which of the following maneuvers will increase the murmur?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app