
Cardiology — MCQs

On this page
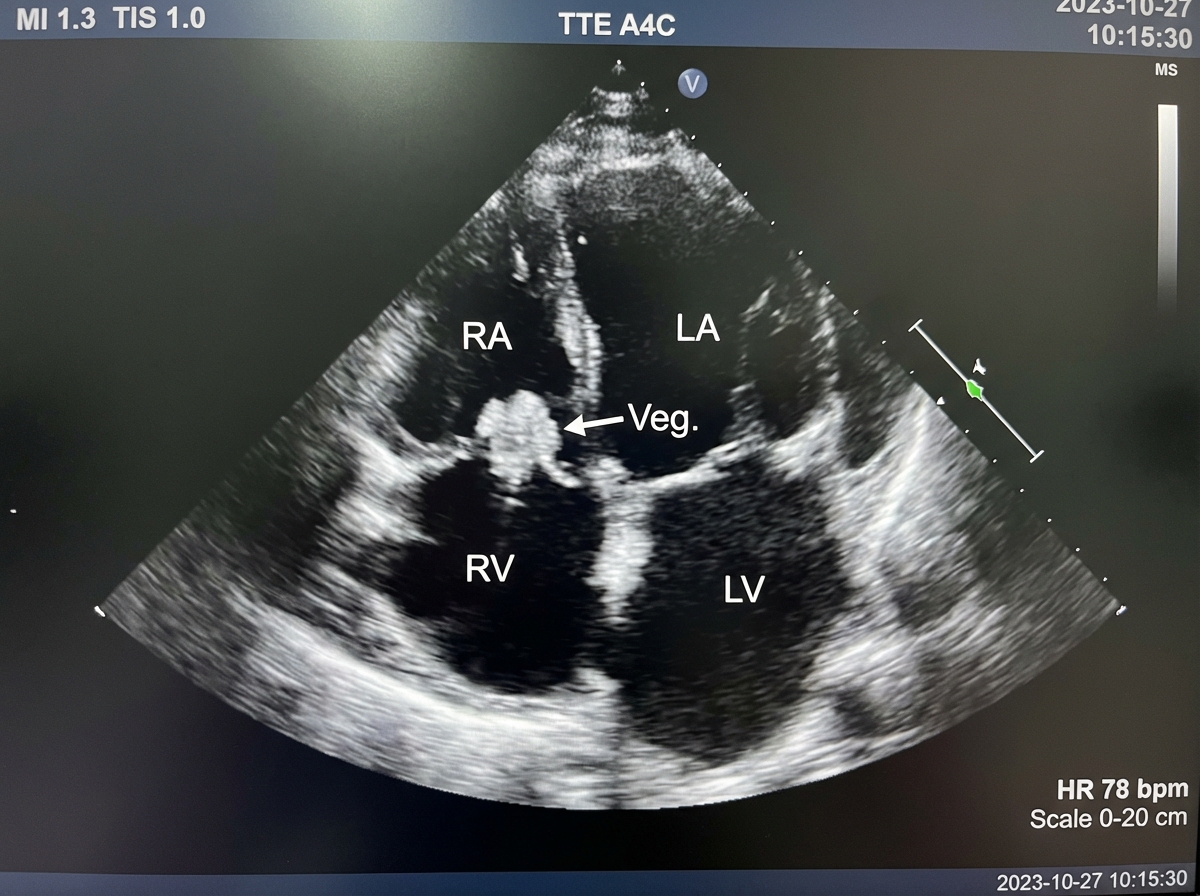
A 27-year-old man from Southern California presents with progressive chest pain, non-productive cough, and shortness of breath for the past 24 hours. He denies any similar symptoms in the past. He denies any family history of cardiac disease, recent travel, or exposure to sick contacts. His temperature is 38.5°C (101.3°F), pulse is 105/min, blood pressure is 108/78 mm Hg, and the respiratory rate is 32/min. On physical examination, patient is cachectic and ill-appearing. Bilateral pleural friction rubs are present on pulmonary auscultation. Antecubital track marks are noted bilaterally. An echocardiogram is performed and results are shown below. Which of the following is the most likely diagnosis in this patient?
A 19-year-old man presents to the emergency department after 2 separate episodes of loss of consciousness. The first episode occurred 1 year ago while he was running in gym class. Witnesses reported clenching and shaking of both hands after he had fallen. On getting up quickly, he felt lightheaded, nauseated, and sweaty. He was given intravenous phenytoin because of concern that he may have had a seizure. His electroencephalogram was negative, and he was not started on long-term antiepileptics. One year later, a second episode of loss of consciousness occurred while playing dodgeball. He experienced a similar prodrome of lightheadedness and sweating. He has no history of seizures outside of these 2 episodes. Family history is non-contributory. He has a temperature of 37.0°C (98.6°F), a blood pressure of 110/72 mm Hg, and a pulse of 80/min. Physical examination is unremarkable. His 12-lead ECG shows normal sinus rhythm without any other abnormalities. Which of the following is the best next step in this patient?
A 35-year-old woman is brought to the emergency department for a severe, left-sided headache and neck pain that started 24 hours after she completed a half-marathon. Shortly after the headache started, she also had weakness of her right upper extremity and sudden loss of vision in her left eye, which both subsided on her way to the hospital. On arrival, she is alert and oriented to person, place, and time. Her temperature is 37.3°C (99.1°F), pulse is 77/min, respiratory rate is 20/min, and blood pressure is 160/90 mm Hg. Examination shows drooping of the left eyelid and a constricted left pupil. Visual acuity in both eyes is 20/20. There is no swelling of the optic discs. Muscle strength and deep tendon reflexes are normal bilaterally. A noncontrast CT scan of the head shows no abnormalities. Duplex ultrasonography of the neck shows absence of flow in the left internal carotid artery. Administration of which of the following is the most appropriate next step in management?
A 33-year-old Caucasian female presents to her primary care provider for pruritus and shortness of breath. Over the past year, she has experienced mild progressive diffuse pruritus. She also reports that her skin seems "hard" and that it has been harder to move her fingers freely. She initially attributed her symptoms to stress at work as a commercial pilot, but when her symptoms began impacting her ability to fly, she decided to seek treatment. She has a history of major depressive disorder and takes citalopram. She smokes 1 pack per day and drinks socially. Her temperature is 98.6°F (37°C), blood pressure is 148/88 mmHg, pulse is 83/min, and respirations are 21/min. On exam, she appears anxious with increased work of breathing. Dry rales are heard at her lung bases bilaterally. Her fingers appear shiny and do not have wrinkles on the skin folds. A normal S1 and S2 are heard on cardiac auscultation. This patient's condition is most strongly associated with which of the following antibodies?
A 22-year-old woman comes to the physician because of 1 week of progressive left anterior knee pain. The pain is worse after sitting for a prolonged period of time and while ascending stairs. She first noticed the pain the day after a basketball game. She has often taken painful blows to the side of the knees while playing basketball but does not recall this having happened in the last game. Four weeks ago, she was diagnosed with a chlamydial urinary tract infection and treated with azithromycin. She is sexually active with one male partner; they use condoms inconsistently. Her vital signs are within normal limits. She is 178 cm (5 ft 10 in) tall and weighs 62 kg (137 lb); BMI is 19.6 kg/m2. Physical examination shows tenderness over the left anterior knee that is exacerbated with anterior pressure to the patella when the knee is fully extended; there is no erythema or swelling. Which of the following is the most likely diagnosis?
A 30-year-old woman comes to the physician because of increased urinary frequency over the past month. She also reports having dry mouth and feeling thirsty all the time despite drinking several liters of water per day. She has not had any weight changes and her appetite is normal. She has a history of obsessive compulsive disorder treated with citalopram. She drinks 1–2 cans of beer per day. Her vital signs are within normal limits. Physical examination shows no abnormalities. Laboratory studies show: Serum Na+ 130 mEq/L Glucose 110 mg/dL Osmolality 265 mOsmol/kg Urine Osmolality 230 mOsmol/kg The patient is asked to stop drinking water for 3 hours. Following water restriction, urine osmolality is measured every hour, whereas serum osmolality is measured every 2 hours. Repeated laboratory measurements show a serum osmolality of 280 mOsmol/kg and a urine osmolality of 650 mOsmol/kg. Which of the following is the most likely diagnosis?
A 41-year-old woman comes to the physician because of a 3-month history of anxiety, difficulty falling asleep, heat intolerance, and a 6-kg (13.2-lb) weight loss. The patient's nephew, who is studying medicine, mentioned that her symptoms might be caused by a condition that is due to somatic activating mutations of the genes for the TSH receptor. Examination shows warm, moist skin and a 2-cm, nontender, subcutaneous mass on the anterior neck. Which of the following additional findings should most raise concern for a different underlying etiology of her symptoms?
A 65-year-old man comes to the physician because of double vision that began this morning. He has hypertension and type 2 diabetes mellitus. He has smoked two packs of cigarettes daily for 40 years. His current medications include lisinopril, metformin, and insulin. Physical examination shows the right eye is abducted and depressed with slight intorsion. Visual acuity is 20/20 in both eyes. Extraocular movements of the left eye are normal. Serum studies show a hemoglobin A1c of 11.5%. Which of the following additional findings is most likely in this patient?
Immediately after undergoing a right total knee replacement, a 69-year-old woman has severe abdominal pain, non-bloody emesis, and confusion. She has a history of Hashimoto thyroiditis that is well-controlled with levothyroxine and hyperlipidemia that is controlled by diet. She underwent bunion removal surgery from her right foot 10 years ago. Her temperature is 39°C (102.2°F), pulse is 120/min, and blood pressure is 60/30 mm Hg. Abdominal examination shows a diffusely tender abdomen with normal bowel sounds. She is confused and oriented to person but not place or time. Laboratory studies are pending. Which of the following is the most appropriate next step in the management of this patient?
A 62-year-old man comes to the physician because of painless swelling in his left foot for 4 months. The swelling was initially accompanied by redness, which has since resolved. He has not had fever or chills. He has a history of coronary artery disease, hyperlipidemia, and type 2 diabetes mellitus. He has had 3 sexual partners over the past year and uses condoms inconsistently. His mother had rheumatoid arthritis. Current medications include clopidogrel, aspirin, metoprolol, losartan, atorvastatin, and insulin. He is 180 cm (5 ft 11 in) tall and weighs 95 kg (209 lb); BMI is 29 kg/m2. Vital signs are within normal limits. Cardiovascular examination shows no abnormalities. Examination of the feet shows swelling of the left ankle with collapse of the midfoot arch and prominent malleoli. There is no redness or warmth. There is a small, dry ulcer on the left plantar surface of the 2nd metatarsal. Monofilament testing shows decreased sensation along both feet up to the shins bilaterally. His gait is normal. Which of the following is the most likely diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app