
Cardiology — MCQs

On this page
A 45-year-old woman diagnosed with a meningioma localized to the tuberculum sellae undergoes endonasal endoscopic transsphenoidal surgery to resect her tumor. Although the surgery had no complications and the patient is recovering well with no neurological sequelae, she develops intense polydipsia and polyuria. Her past medical history is negative for diabetes mellitus, cardiovascular disease, or malignancies. Urine osmolality is 240 mOsm/L (300–900 mOsm/L), and her serum sodium level is 143 mEq/L (135–145 mEq/L). The attending decides to perform a water deprivation test. Which of the following results would you expect to see after the administration of desmopressin in this patient?
A 46-year-old woman comes to the physician because of increasingly severe lower back pain for the past week. The pain is constant, and she describes it as 9 out of 10 in intensity. Six months ago, she underwent a lumpectomy for hormone receptor-negative lobular carcinoma of the right breast. She has undergone multiple cycles of radiotherapy. Vital signs are within normal limits. Examination shows a well-healed surgical incision over the right breast. There is severe tenderness to palpation over the 12th thoracic vertebra. The straight-leg raise test is negative. The remainder of the examination shows no abnormalities. Serum studies show: Glucose 76 mg/dL Creatinine 1 mg/dL Total bilirubin 0.8 mg/dL Alkaline phosphatase 234 U/L Aspartate aminotransferase (AST, GOT) 16 U/L Alanine aminotransferase (ALT, GPT) 12 U/L γ-Glutamyltransferase (GGT) 40 U/L (N=5–50) Which of the following is the most appropriate next step in management?
A 37-year-old woman comes to the physician for a 6-month history of headaches, anorexia, and vomiting. She has had a 10-kg (22-lb) weight loss during this period. She has type 1 diabetes mellitus for which she takes insulin. The patient's mother and sister have hypothyroidism. Her blood pressure is 80/60 mm Hg. Physical examination shows hyperpigmentation of the lips and oral mucosa. Serum studies show a parathyroid hormone level of 450 pg/mL and antibodies directed against 21-hydroxylase. Which of the following is the most likely diagnosis?
A 53-year-old diabetic man with cellulitis of the right lower limb presents to the emergency department because of symptoms of fever and chills. His pulse is 122/min, the blood pressure is 76/50 mm Hg, the respirations are 26/min, and the temperature is 40.0°C (104.0°F). His urine output is < 0.5mL/kg/h. He has warm peripheral extremities. The hemodynamic status of the patient is not improving in spite of the initiation of adequate fluid resuscitation. He is admitted to the hospital. Which of the following is the most likely laboratory profile?
A day after percutaneous coronary intervention for stable angina, a 63-year-old woman develops severe pain in her right small toe. She has no history of a similar episode. She has had diabetes mellitus for 16 years. After the procedure, her blood pressure is 145/90 mm Hg, the pulse is 65/min, the respiratory rate is 15/min, and the temperature is 36.7°C (98.1°F). Physical examination of the femoral artery access site shows no abnormalities. Distal pulses are palpable and symmetric. A photograph of the toe is shown. Which of the following is the most likely diagnosis?

A 45-year-old African American woman presents to her primary care physician for not feeling well. She states she has had a cough for the past week. In addition, she also has abdominal pain and trouble focusing that has been worsening. She states that she has also lost 5 pounds recently and that her gastroesophageal reflux disease (GERD) has been very poorly controlled recently. The patient is a non-smoker and has a history of GERD for which she takes antacids. Laboratory studies are ordered and are below: Serum: Na+: 139 mEq/L K+: 4.1 mEq/L Cl-: 101 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 12 mg/dL Glucose: 70 mg/dL Creatinine: 0.9 mg/dL Ca2+: 12.5 mg/dL Alkaline phosphatase: 35 U/L Phosphorus: 2.0 mg/dL Urine: Color: amber Nitrites: negative Sodium: 5 mmol/24 hours Red blood cells: 0/hpf Which of the following is the most likely explanation of this patient's current presentation?
A 27-year-old woman is admitted to the emergency room with dyspnea which began after swimming and progressed gradually over the last 3 days. She denies cough, chest pain, or other respiratory symptoms. She reports that for the past 4 months, she has had several dyspneic episodes that occurred after the exercising and progressed at rest, but none of these were as long as the current one. Also, she notes that her tongue becomes ‘wadded’ when she speaks and she tires very quickly during the day. The patient’s vital signs are as follows: blood pressure 125/60 mm Hg, heart rate 92/min, respiratory rate 34/min, and body temperature 36.2℃ (97.2℉). Blood saturation on room air is initially 92% but falls to 90% as she speaks up. On physical examination, the patient is slightly lethargic. Her breathing is rapid and shallow. Lung auscultation, as well as cardiac, and abdominal examinations show no remarkable findings. Neurological examination reveals slight bilateral ptosis increased by repetitive blinking, and easy fatigability of muscles on repeated movement worse on the face and distal muscles of the upper and lower extremities. Which arterial blood gas parameters would you expect to see in this patient?
A 47-year-old woman presents to her primary care physician because of pain on urination, urinary urgency, and urinary frequency for 4 days. This is the third time for her to have these symptoms over the past 7 months. She was recently treated for candidal intertrigo. Vital signs reveal a temperature of 36.7°C (98.0°F), blood pressure of 110/70 mm Hg and pulse of 75/min. Physical examination is unremarkable except for morbid obesity. Her father has type 2 diabetes complicated by end-stage chronic kidney disease. A1C is found to be 8.5%. The patient is given a prescription for her urinary symptoms. Which of the following is the best next step for this patient?
A 59-year-old man presents to his family practitioner with his wife. He has fallen several times over the past 3 months. Standing up from a seated position is especially difficult for him. He also complains of intermittent dizziness, excessive sweating, constipation, and difficulty performing activities of daily living. He denies fever, jerking of the limbs, memory disturbances, urinary incontinence, and abnormal limb movements. Past medical history includes a cholecystectomy 25 years ago and occasional erectile dysfunction. He takes a vitamin supplement with calcium and occasionally uses sildenafil. While supine, his blood pressure is 142/74 mm Hg and his heart rate is 64/min. After standing, his blood pressure is 118/60 mm Hg and his heart rate is 62/min. He is alert and oriented with a flat affect while answering questions. Extraocular movements are intact in all directions. No tremors are noticed. Muscle strength is normal in all limbs but with increased muscle tone. He is slow in performing intentional movements. His writing is small and he takes slow steps during walking with adducted arms and a slightly reduced arm swing. A trial of levodopa did not improve his symptoms. What is the most likely diagnosis?
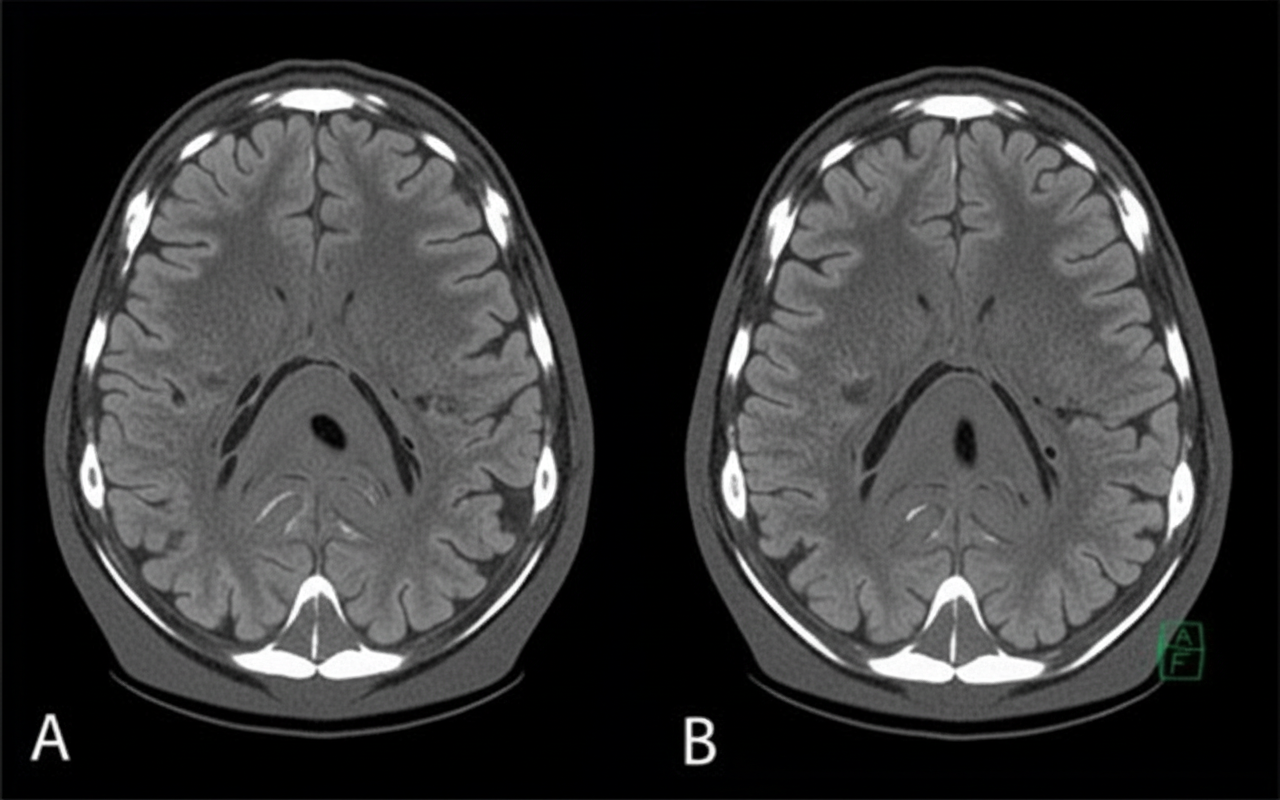
A 58-year-old man presents to the clinic concerned about his health after his elder brother recently became bed-bound due to cerebral small vessel disease/vascular cognitive impairment. He has also brought a head CT scan of his brother to reference, as shown in the picture. The patient has type 2 diabetes mellitus, hypertension, osteoarthritis, and hypercholesterolemia. His medication list includes aspirin, diclofenac sodium, metformin, and ramipril. He leads a sedentary lifestyle and smokes one pack of cigarettes daily. He also drinks 4–5 cups of red wine every weekend. His BMI is 33.2 kg/m2. His blood pressure is 164/96 mm Hg, the heart rate is 84/min, and the respiratory rate is 16/min. Which of the following interventions will be most beneficial for reducing the risk of developing the disease that his brother has?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app