
Cardiology — MCQs

On this page
A 38-year-old woman comes to the physician because of a 1-month history of progressively worsening dyspnea, cough, and hoarseness of voice. Her pulse is 92/min and irregularly irregular, respirations are 20/min, and blood pressure is 110/75 mm Hg. Cardiac examination shows a rumbling mid-diastolic murmur that is best heard at the apex in the left lateral decubitus position. Which of the following is the most likely underlying cause of this patient's condition?
A 44-year-old woman comes to the physician because of progressively worsening shortness of breath with exertion and intermittent palpitations over the last 2 months. She has had neither chest pain nor a cough. Her pulse is 124/min and irregular. Physical examination shows a grade 4/6 high-pitched holosystolic murmur that is best heard at the apex and radiates to the back. The murmur increases in intensity when she clenches her hands into fists. The lungs are clear to auscultation. Further evaluation of this patient is most likely to show which of the following findings?
A 57-year-old woman comes to the clinic complaining of decreased urine output. She reports that over the past 2 weeks she has been urinating less and less every day. She denies changes in her diet or fluid intake. The patient has a history of lupus nephritis, which has resulted in end stage renal disease. She underwent a renal transplant 2 months ago. Since then she has been on mycophenolate and cyclosporine, which she takes as prescribed. The patient’s temperature is 99°F (37.2°C), blood pressure is 172/102 mmHg, pulse is 88/min, and respirations are 17/min with an oxygen saturation of 97% on room air. Labs show an elevation in serum creatinine and blood urea nitrogen. On physical examination, she has 2+ pitting edema of the bilateral lower extremities. Lungs are clear to auscultation. Urinalysis shows elevated protein. A post-void bladder scan is normal. A renal biopsy is obtained, which shows lymphocyte infiltration and intimal swelling. Which of the following is the next best step in management?
A 68-year-old female presents to your office for her annual check-up. Her vitals are HR 85, T 98.8 F, RR 16, BP 125/70. She has a history of smoking 1 pack a day for 35 years, but states she quit five years ago. She had her last pap smear at age 64 and states all of her pap smears have been normal. She had her last colonoscopy at age 62, which was also normal. Which of the following is the next best test for this patient?
A 72-year-old woman is brought to the emergency department because of lethargy and weakness for the past 5 days. During this period, she has had a headache that worsens when she leans forward or lies down. Her arms and face have appeared swollen over the past 2 weeks. She has a history of hypertension and invasive ductal carcinoma of the left breast. She underwent radical amputation of the left breast followed by radiation therapy 4 years ago. She has smoked two packs of cigarettes daily for 40 years. Current medications include aspirin, hydrochlorothiazide, and tamoxifen. Her temperature is 37.2°C (99°F), pulse is 103/min, and blood pressure is 98/56 mm Hg. Examination shows jugular venous distention, a mastectomy scar over the left thorax, and engorged veins on the anterior chest wall. There is no axillary or cervical lymphadenopathy. There is 1+ pitting edema in both arms. Which of the following is the most likely cause of this patient's symptoms?
A 65-year-old male with a history of coronary artery disease and myocardial infarction status post coronary artery bypass graft (CABG) surgery presents to his cardiologist for a routine appointment. On physical exam, the cardiologist appreciates a holosystolic, high-pitched blowing murmur heard loudest at the apex and radiating towards the axilla. Which of the following is the best predictor of the severity of this patient's murmur?
A 20-year-old man presents to the emergency department. The patient was brought in by his coach after he fainted during a competition. This is the second time this has happened since the patient joined the track team. The patient has a past medical history of multiple episodes of streptococcal pharyngitis which were not treated in his youth. He is not currently on any medications. He is agreeable and not currently in any distress. His temperature is 99.5°F (37.5°C), blood pressure is 132/68 mmHg, pulse is 90/min, respirations are 12/min, and oxygen saturation is 98% on room air. On physical exam, you note a young man in no current distress. Neurological exam is within normal limits. Pulmonary exam reveals clear air movement bilaterally. Cardiac exam reveals a systolic murmur best heard at the lower left sternal border that radiates to the axilla. Abdominal exam reveals a soft abdomen that is non-tender in all 4 quadrants. The patient's cardiac exam is repeated while he squats. Which of the following is most likely true for this patient?
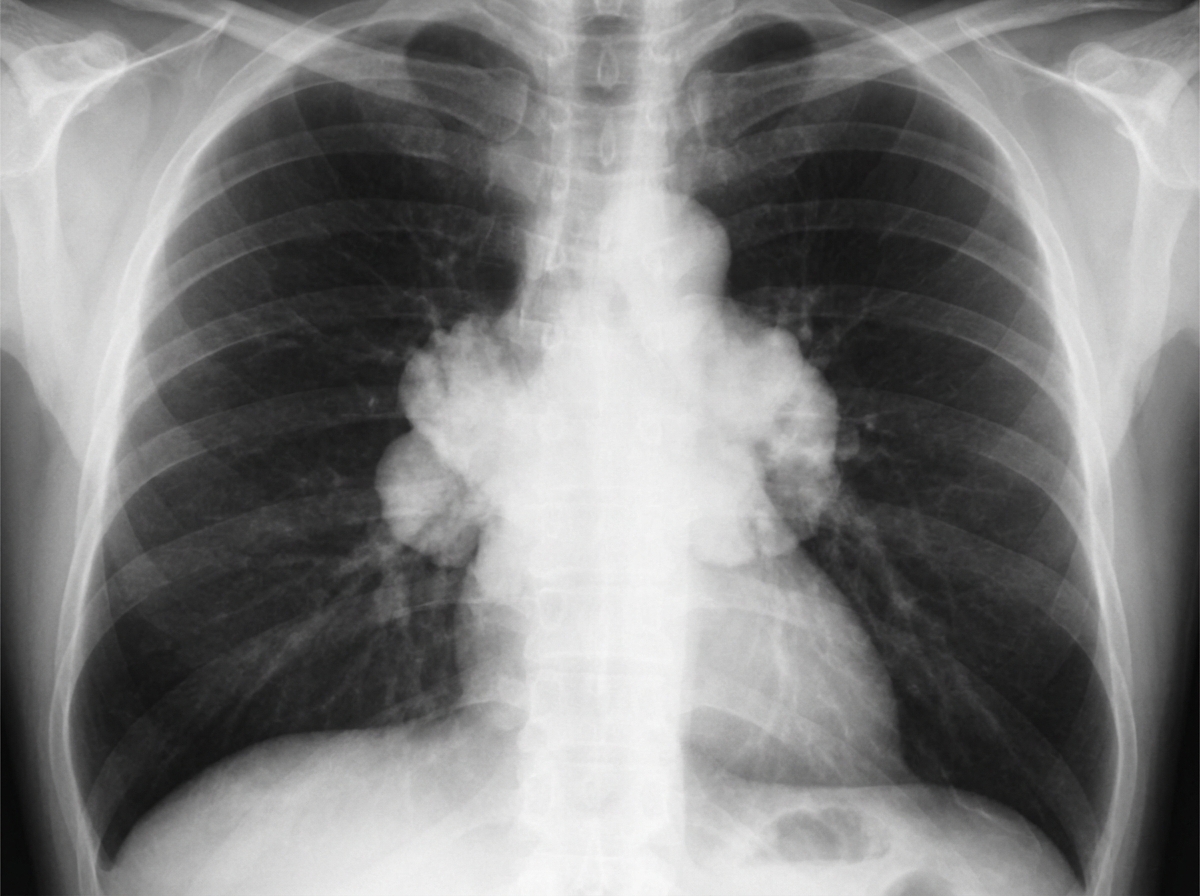
A 67-year-old man presents to his primary care physician because of a dry cough and shortness of breath for 2 months. He notes that recently he has had easy bruising of the skin without obvious trauma. He has a past history of chronic obstructive pulmonary disease and recently diagnosed with type 2 diabetes. Family history is non-contributory. He has smoked 1 pack of cigarettes daily for 35 years but quit 3 years ago. His temperature is 37.1°C (98.7°F), blood pressure is 170/80 mm Hg, and pulse is 85/min. On physical examination, the patient's face is round and plethoric and there are large supraclavicular fat pads. Breath sounds are diminished all over the chest without focal rales or wheezes. Chest X-ray is shown in the picture. Which of the following is the most likely etiology of this patient's condition?
A 56-year-old man presents to the physician for the evaluation of excess snoring over the past year. He has no history of a serious illness and takes no medications. He does not smoke. His blood pressure is 155/95 mm Hg. BMI is 49 kg/m2. Oropharyngeal examination shows an enlarged uvula. Examination of the nasal cavity shows no septal deviation or polyps. Examination of the lungs and heart shows no abnormalities. Polysomnography shows an apnea-hypopnea index of 2 episodes/h with a PCO2 of 51 mm Hg during REM sleep. Arterial blood gas analysis in room air shows: pH 7.33 PCO2 50 mm Hg PO2 92 mm Hg HCO3− 26 mEq/L Which of the following best explains these findings?
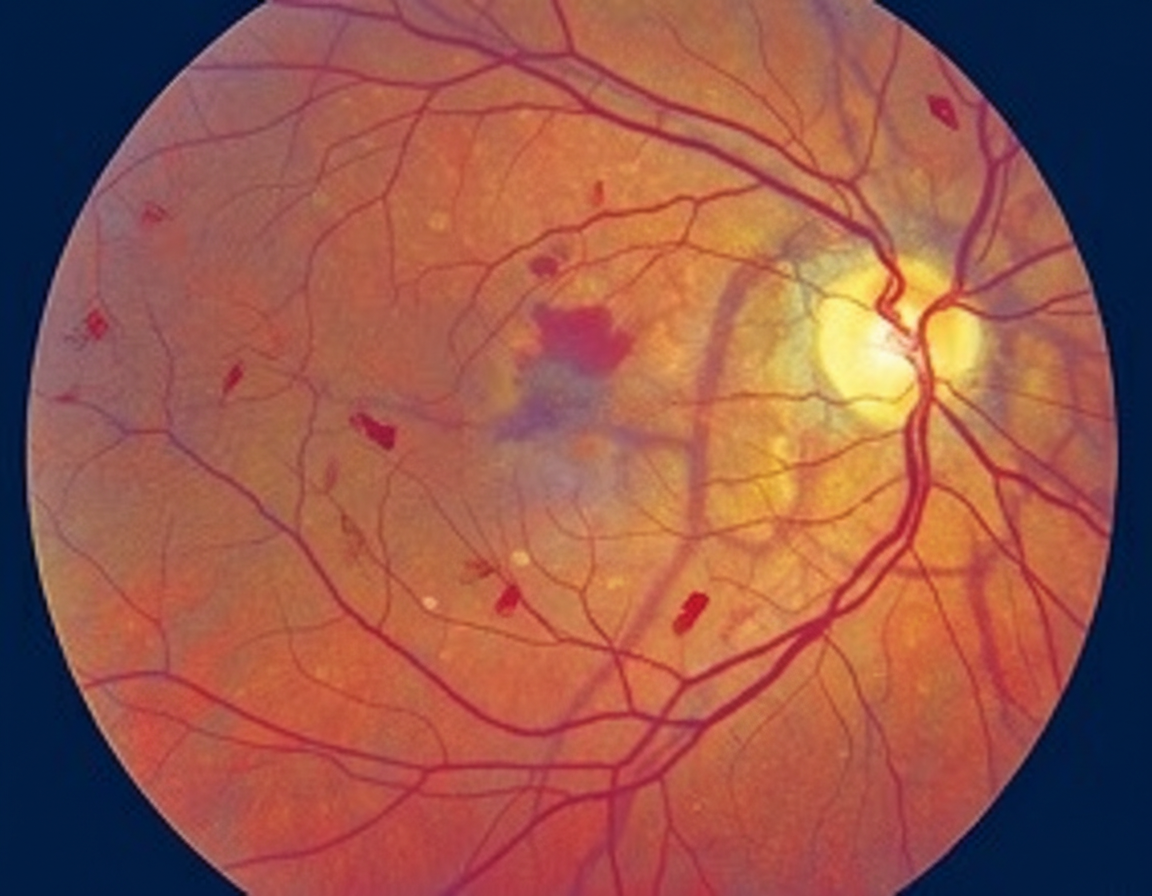
A 55-year-old woman comes to the physician because of increased blurring of vision in both eyes for the past 4 months. She has tried using over-the-counter reading glasses, but they have not helped. She has a history of hypertension, type 2 diabetes mellitus, and chronic obstructive pulmonary disease. Current medications include lisinopril, insulin, metformin, and a fluticasone-vilanterol inhaler. Vital signs are within normal limits. Examination shows visual acuity of 20/70 in each eye. A photograph of the fundoscopic examination of the right eye is shown. Optical coherence tomography (OCT) confirms center-involving diabetic macular edema with subretinal fluid and increased central macular thickness. Which of the following is the most appropriate next step in management?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app