
Cardiology — MCQs

On this page
Four days after undergoing an elective total hip replacement, a 65-year-old woman develops a DVT that embolizes to the lung. Along with tachypnea, tachycardia, and cough, the patient would most likely present with a PaO2 of what?
A 33-year-old man comes to the physician because of gradually worsening bilateral foot pain for 2 months. The pain used to only occur after long walks and subside with rest. For the past week, the pain has been continuous and associated with burning sensations. He has also had transient painful nodules along the course of the leg veins for 4 months that resolve spontaneously. The patient is wearing an ankle brace for support because of a sprained left ankle that occurred three months ago. His mother was diagnosed with protein C deficiency as a teenager. He has smoked 2 packs of cigarettes daily for 15 years and does not drink alcohol. Vitals signs are within normal limits. Examination shows ulcers on the distal portion of his left great, second, and fifth toes. The feet are cool. Pedal pulses are barely palpable. Ankle-brachial pressure index is 0.3 in the left leg and 0.5 in the right leg. Which of the following interventions is most likely to reduce the risk of amputation in this patient?
A 67-year-old woman is brought by ambulance from home to the emergency department after she developed weakness of her left arm and left face droop. According to her husband, she has a history of COPD, hypertension, and hyperlipidemia. She takes hydrochlorothiazide, albuterol, and atorvastatin. She is not on oxygen at home. She is an active smoker and has smoked a pack a day for 20 years. Her mother died of a heart attack at age 60 and her father died of prostate cancer at age 55. By the time the ambulance arrived, she was having difficulty speaking. Once in the emergency department, she is no longer responsive. Her blood pressure is 125/85 mm Hg, the temperature is 37.2°C (99°F), the heart rate is 77/min, and her breathing is irregular, and she is taking progressively deeper inspirations interrupted with periods of apnea. Of the following, what is the next best step?
A 64-year-old woman is brought to the emergency department 1 hour after the onset of acute shortness of breath and chest pain. The chest pain is retrosternal in nature and does not radiate. She feels nauseated but has not vomited. She has type 2 diabetes mellitus, hypertension, and chronic kidney disease. Current medications include insulin, aspirin, metoprolol, and hydrochlorothiazide. She is pale and diaphoretic. Her temperature is 37°C (98°F), pulse is 136/min, and blood pressure is 80/60 mm Hg. Examination shows jugular venous distention and absence of a radial pulse during inspiration. Crackles are heard at the lung bases bilaterally. Cardiac examination shows distant heart sounds. Laboratory studies show: Hemoglobin 8.3 g/dL Serum Glucose 313 mg/dL Urea nitrogen 130 mg/dL Creatinine 6.0 mg/dL Which of the following is the most appropriate next step in management?
A 35-year-old female comes to the physician because of a 2-year history of progressive fatigue and joint pain. She has a 1-year history of skin problems and a 4-month history of episodic pallor of her fingers. She reports that the skin of her face, neck, and hands is always dry and itchy; there are also numerous “red spots” on her face. She has become more “clumsy” and often drops objects. She has gastroesophageal reflux disease treated with lansoprazole. She does not smoke. She occasionally drinks a beer or a glass of wine. Her temperature is 36.5°C (97.7°F), blood pressure is 154/98 mm Hg, and pulse is 75/min. Examination shows hardening and thickening of the skin of face, neck, and hands. There are small dilated blood vessels around her mouth and on her oral mucosa. Mouth opening is reduced. Active and passive range of motion of the proximal and distal interphalangeal joints is limited. Cardiopulmonary examination shows no abnormalities. Her creatinine is 1.4 mg/dL. The patient is at increased risk for which of the following complications?
A 16-year-old girl is brought to the physician because of a 6-month history of menstrual cramps, heavy menstrual flow, and fatigue; she has gained 5 kg (11 lb) during this period. Menses occur at regular 30-day intervals and last 8 to 10 days; during her period she uses 7 tampons a day and is unable to participate in any physical activities because of cramping. Previously, since menarche at the age of 11 years, menses had lasted 4 to 5 days with moderate flow. Her last menstrual period was 3 weeks ago. She has limited scleroderma with episodic pallor of the fingertips. She takes no medications. She is 160 cm (5 ft 3 in) tall and weighs 77 kg (170 lb); BMI is 30 kg/m2. Her temperature is 36.5°C (97.7°F), pulse is 56/min, respirations are 16/min, and blood pressure is 100/65 mm Hg. Physical examination shows a puffy face with telangiectasias and thinning of the eyebrows. Deep tendon reflexes are 1+ bilaterally with delayed relaxation. Pelvic examination shows a normal appearing vagina, cervix, uterus, and adnexa. Further evaluation of this patient is most likely to show which of the following findings?
A 32-year-old man presents with hypertension that has been difficult to control with medications. His symptoms include fatigue, frequent waking at night for voiding, and pins and needles in the legs. His symptoms started 2 years ago. Family history is positive for hypertension in his mother. His blood pressure is 160/100 mm Hg in the right arm and 165/107 mm Hg in the left arm, pulse is 85/min, and temperature is 36.5°C (97.7°F). Physical examination reveals global hyporeflexia and muscular weakness. Lab studies are shown: Serum sodium 147 mEq/L Serum creatinine 0.7 mg/dL Serum potassium 2.3 mEq/L Serum bicarbonate 34 mEq/L Plasma renin activity low Which of the following is the most likely diagnosis?
A 30-year-old man comes to the clinic with complaints of increased frequency of urination, especially at night, for about a month. He has to wake up at least 5-6 times every night to urinate and this is negatively affecting his sleep. He also complains of increased thirst and generalized weakness. Past medical history is significant for bipolar disorder. He is on lithium which he takes regularly. Blood pressure is 150/90 mm Hg, pulse rate is 80/min, respiratory rate is 16/min, and temperature is 36°C (96.8°F). Physical examination is normal. Laboratory studies show: Na+: 146 mEq/L K+: 3.8 mEq/L Serum calcium: 9.5 mg/dL Creatinine: 0.9 mg/dL Urine osmolality: 195 mOsm/kg Serum osmolality: 305 mOsm/kg Serum fasting glucose: 90 mg/dL Which of the following is the best initial test for the diagnosis of his condition?
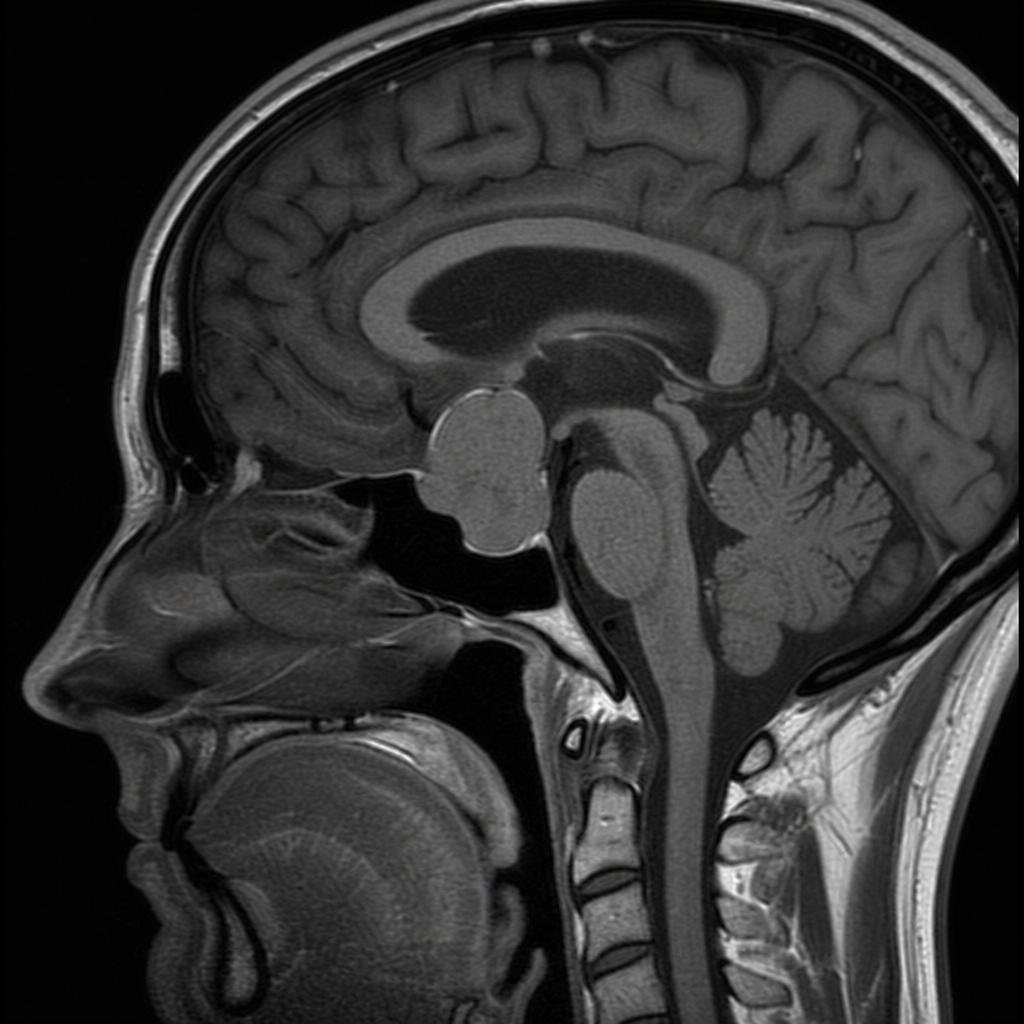
A 47-year-old taxi driver visits an ophthalmologist after failing a routine eye test for his driver's license renewal. The patient reports a slight blurring of his vision, headaches, and occasional dizziness for the past month. On further questioning, he admits to feeling tired and out of sorts most of the time. He attributes it to working overtime and experiencing stress at home. He also complains of decreased libido, decreased appetite, and some weight loss over the past 2 months. There is no history of cold intolerance or hoarseness of voice. On examination, the patient appears malnourished. His vital signs are within normal limits. On physical examination, his thyroid gland is firm and normal in size. Genital examination reveals small, soft testes with patchy pubic hair. Ophthalmic examination reveals decreased visual acuity. His laboratory results are significant for decreased serum ACTH, decreased serum cortisol, normal serum TSH, normal serum T4, decreased serum LH, decreased serum FSH, and decreased serum GH. On suspicions raised by the patient's physical examination and lab studies, the clinician orders a brain MRI. The scan shows a pituitary macroadenoma impinging on and displacing the optic chiasm. Which of the following is the most likely diagnosis?
A 29-year-old homeless man visits his local walk-in-clinic complaining of shortness of breath, fatigability, malaise, and fever for the past month. His personal history is significant for multiple inpatient psychiatric hospitalizations for a constellation of symptoms that included agitation, diarrhea, dilated pupils, and restless legs. On physical examination, his blood pressure is 126/72 mm Hg, heart rate is 117/min, body temperature is 38.5°C (101.3°F), and saturating 86% on room air. Auscultation reveals a holosystolic murmur that is best heard at the left sternal border and noticeably enhanced during inspiration. What is the underlying pathophysiological mechanism in this patient’s heart condition?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app