
Cardiology — MCQs

On this page
A 72-year-old man presents to his primary care physician for his annual exam. He has a very stoic personality and says that he is generally very healthy and has "the normal aches and pains of old age." On further probing, you learn that he does have pretty significant back and hip pain that worsens throughout the day. On physical exam you note bony enlargement of the distal interphalangeal joints bilaterally. Which of the following is the likely cause of his symptoms?
A 77-year-old man with a history of hypertension and a 46 pack-year smoking history presents to the emergency department from an extended care facility with acute onset of headache, nausea, vomiting, and neck pain which started 6 hours ago and has persisted since. He is alert, but his baseline level of consciousness is slightly diminished per the nursing home staff. His temperature is 99.0°F (37.2°C), blood pressure is 164/94 mmHg, pulse is 90/min, respirations are 16/min, and oxygen saturation is 98% on room air. The patient's neurological exam is unremarkable with cranial nerves II-XII grossly intact and with stable gait with a walker. He is immediately sent for a head CT which is normal. What is the most appropriate next step in management?
A 42-year-old man with a history of tuberculosis presents to your office complaining of fatigue for two months. Serum laboratory studies reveal the following: WBC 7,000 cells/mm^3, Hb 9.0 g/dL, Hct 25%, MCV 88 fL, Platelet 450,000 cells/mm^3, Vitamin B12 500 pg/mL (200-800), and Folic acid 17 ng/mL (2.5-20). Which of the following is the most appropriate next step in the management of anemia in this patient?
A 15-year-old girl comes to the physician with her father for evaluation of her tall stature. She is concerned because she is taller than all of her friends. Her birth weight and height were within normal limits. Her father is 174 cm (5 ft 7 in) tall; her mother is 162 cm (5 ft 3 in) tall. She is at the 98th percentile for height and 90th percentile for BMI. She has not had her menstrual period yet. Her mother has Graves disease. Vital signs are within normal limits. Examination shows a tall stature with broad hands and feet. There is frontal bossing and protrusion of the mandible. Finger perimetry is normal. The remainder of the examinations shows no abnormalities. Serum studies show a fasting serum glucose of 144 mg/dL. An x-ray of the left hand and wrist shows a bone age of 15 years. Which of the following is the most appropriate definitive treatment for this patient's condition?
A previously healthy 22-year-old man presents to the university clinic with increasing scrotal pain and swelling over the past 5 days. He also has dysuria and urinary frequency. He has never felt this type of pain before. The young man considers himself generally healthy and takes no medications. He is sexually active with one partner and uses condoms inconsistently. At the clinic, his temperature is 36.7℃ (98.1℉), the blood pressure is 115/70 mm Hg, the pulse is 84/min, and the respirations are 14/min. On examination, he has swelling and tenderness of the right scrotum, especially over the posterior aspect of the right testicle. The Prehn sign is positive. The remainder of the physical exam is unremarkable. Doppler sonography shows increased blood flow to the testis. Which of the following is the most appropriate next step in management?
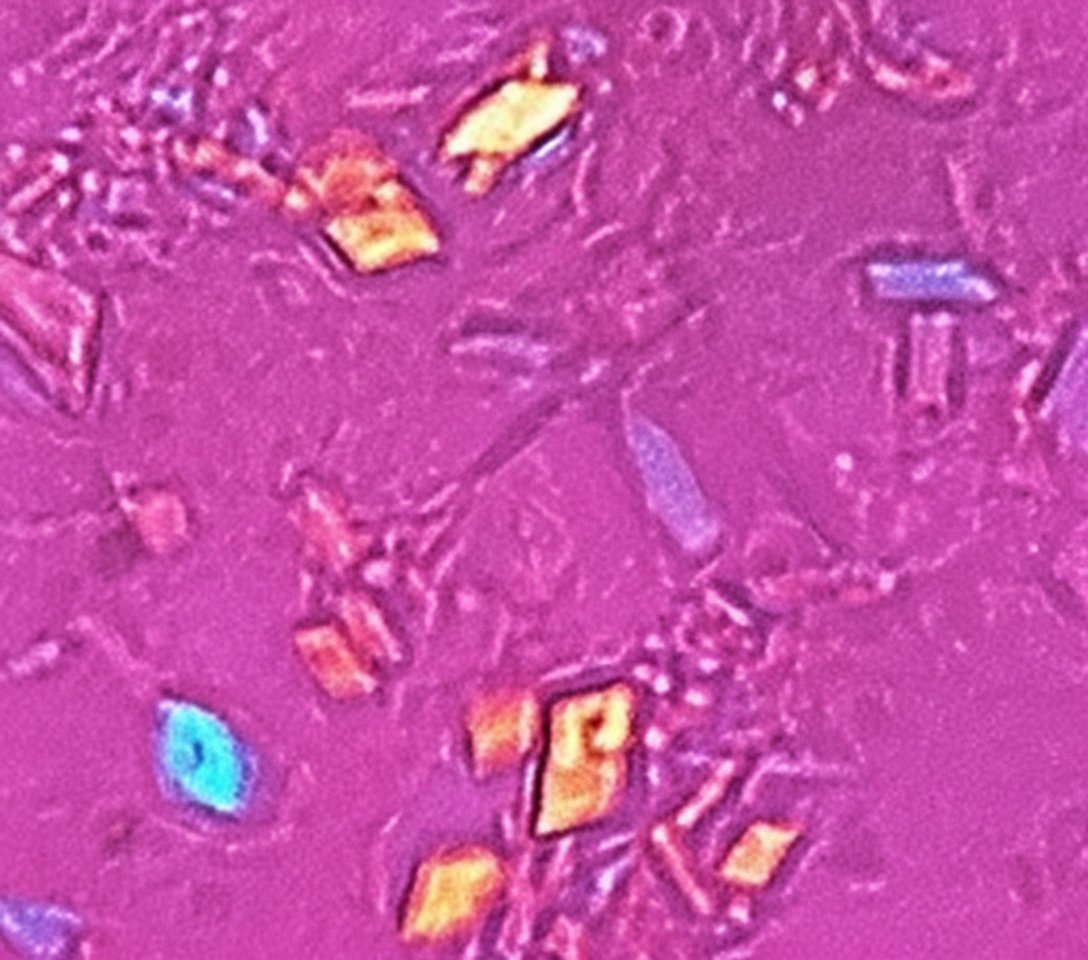
A 54-year-old woman comes to the physician because of constant dull pain, swelling, and progressive stiffness of the right knee for 3 days. Use of over-the-counter analgesics has only provided minimal relief of her symptoms. She has not had any similar symptoms in the past. She takes hydrochlorothiazide for hypertension. Examination of the right knee shows a large effusion and mild erythema. There is moderate tenderness to palpation. Range of motion is limited by pain. Arthrocentesis of the right knee is performed, and microscopic examination of the synovial fluid under polarized light is shown. Further evaluation of this patient is most likely to show which of the following findings?
A 57-year-old man presents to the emergency department after a motor vehicle collision. The patient was the back seat restrained passenger in a vehicle that was rear ended at 25 miles/hour. The patient has a past medical history of diabetes, hypertension, and chronic obstructive pulmonary disease (COPD). His temperature is 97.5°F (36.4°C), blood pressure is 97/68 mmHg, pulse is 130/min, respirations are 22/min, and oxygen saturation is 99% on room air. The patient is subsequently worked up receiving a chest radiograph, ECG, FAST exam, and serum chemistries. A cardiac catheterization reveals equilibration in diastolic pressure across all cardiac chambers. Which of the following is the most likely diagnosis?
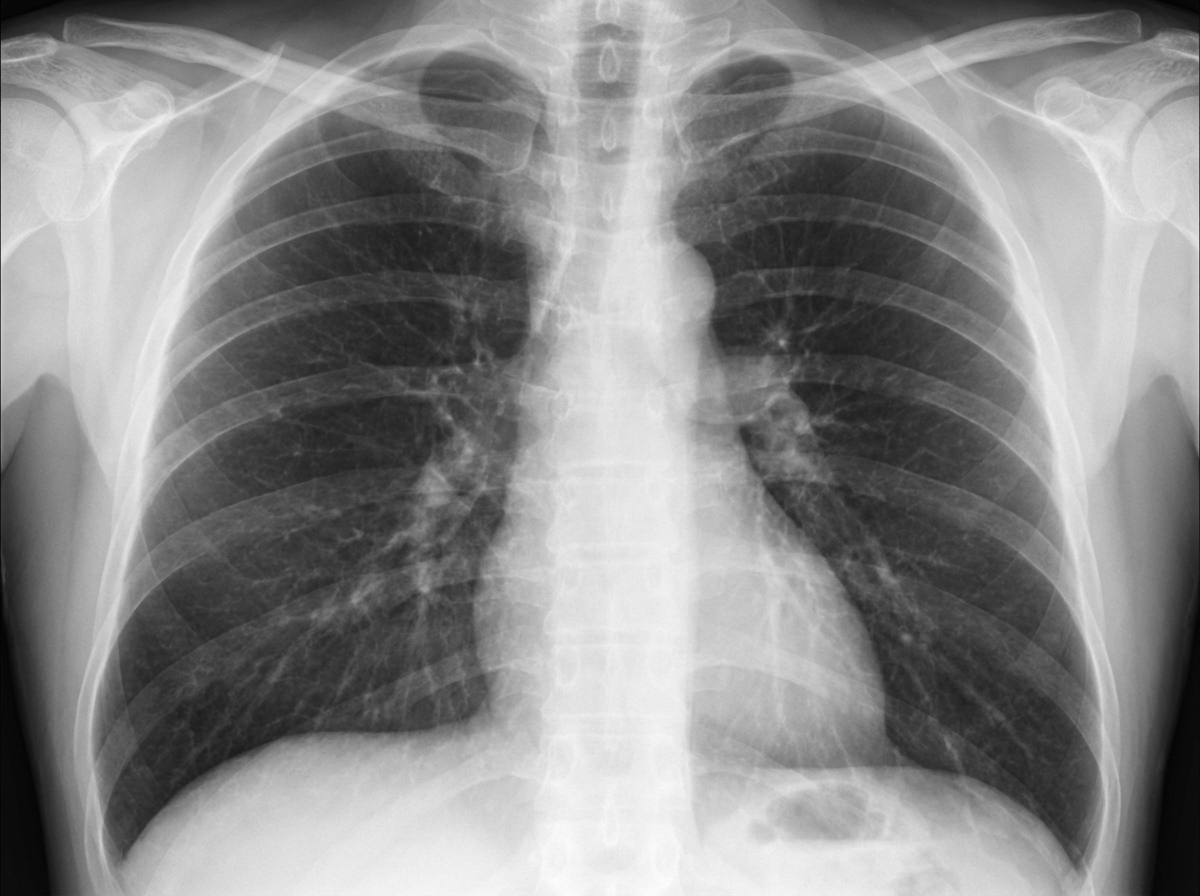
A 36-year-old woman comes to the physician because of a 3-month history of intermittent cough productive of thick, yellow phlegm and increasing shortness of breath. She especially becomes short of breath while playing with her children. She has worked as a farmer for 18 years. She has asthma treated with a salbutamol inhaler. She has smoked half a pack of cigarettes daily for 12 years. Her pulse is 65/min, respirations are 14/min, and blood pressure is 110/75 mm Hg. Scattered wheezing and decreased breath sounds are heard throughout both lung fields. Cardiac examination shows no abnormalities. The abdomen is soft and nondistended; liver span in midclavicular line is 14 cm.Spirometry shows a FEV1:FVC ratio of 66% and a FEV1 of 50% of predicted. An x-ray of the chest is shown. Which of the following is the most likely underlying cause of this patient's condition?
A 72-year-old man comes to the physician for medical clearance for a molar extraction. He feels well. He reports he is able to climb 3 flights of stairs without experiencing any shortness of breath. He has hypertension, type 2 diabetes mellitus, and ischemic heart disease. He underwent an aortic valve replacement for severe aortic stenosis last year and had a prior episode of infective endocarditis 3 years ago. 12 years ago, he underwent a cardiac angioplasty and had 2 stents placed. Current medications include aspirin, warfarin, lisinopril, metformin, sitagliptin, and simvastatin. His temperature is 37.1°C (98.8°F), pulse is 92/min, and blood pressure is 136/82 mm Hg. A systolic ejection click is heard at the right second intercostal space. Which of the following is the most appropriate next step in management?
A 36-year-old man is brought in by ambulance after being found down on the sidewalk. It is uncertain how long he was down before being found, and he did not have any forms of identification when he was found. On presentation, the man is found to still be unconscious with a disheveled and unkempt appearance. He is also found to be taking slow, shallow breaths that smell of alcohol. His temperature is 98.8°F (37.1°C), blood pressure is 106/67 mmHg, pulse is 119/min, respirations are 5/min, and oxygen saturation is 87% on room air. His pupils are found to be fixed and contracted, and he has multiple bruises and scars on his body. Which of the following sets of findings would most likely be seen in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app