
Cardiology — MCQs

On this page
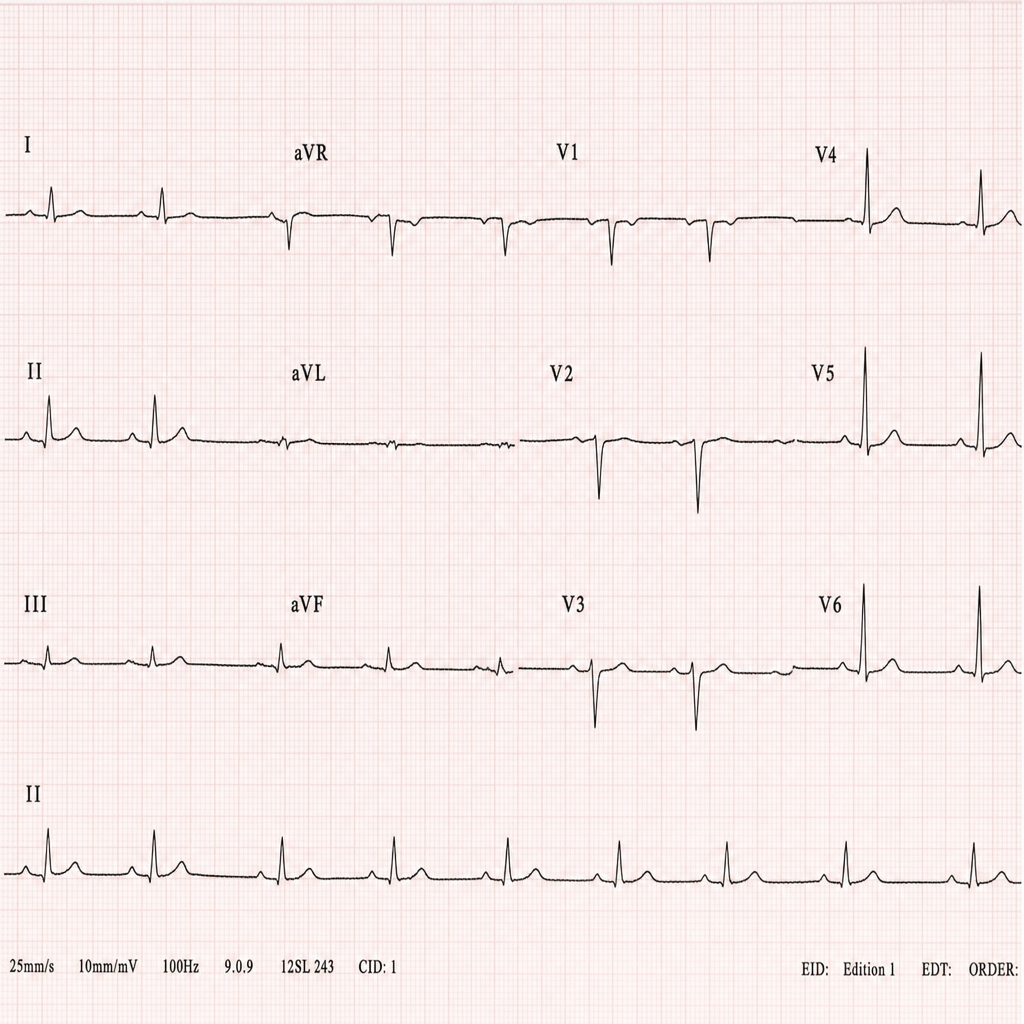
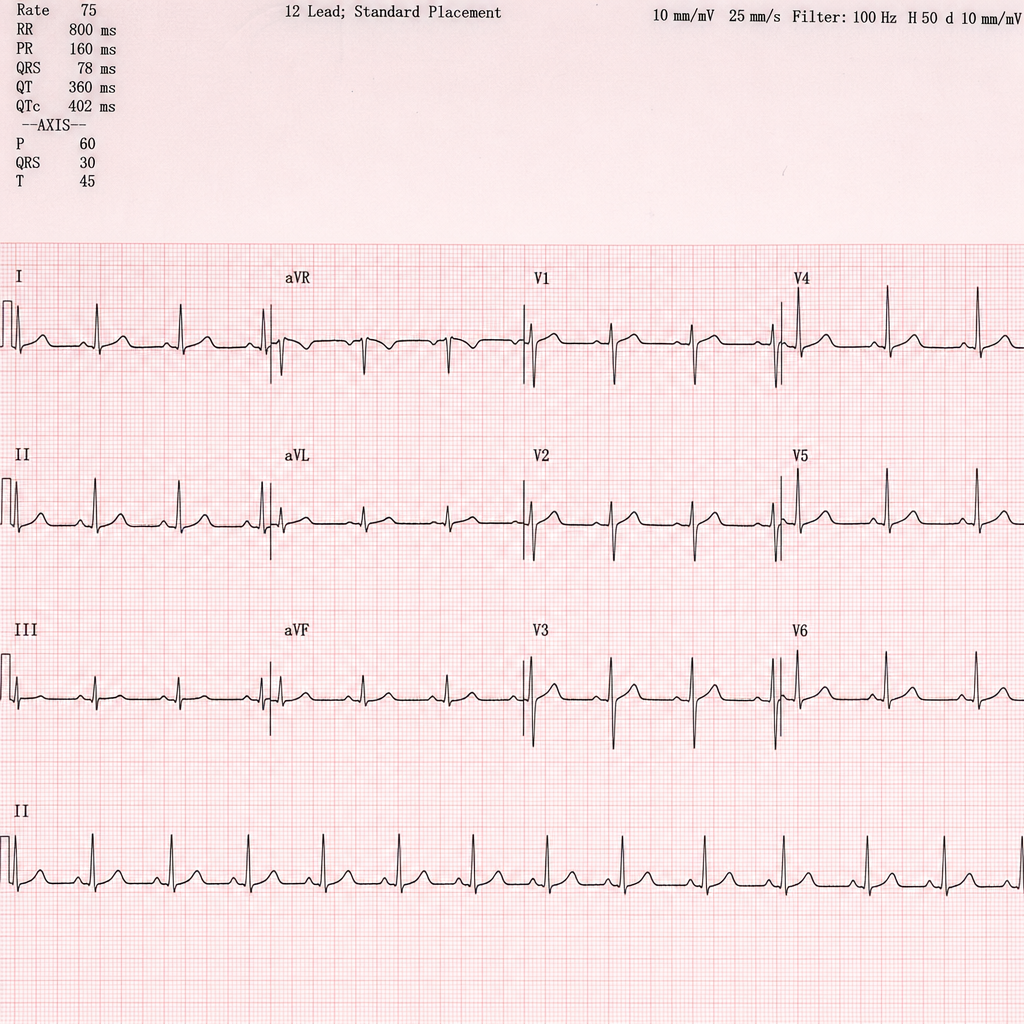
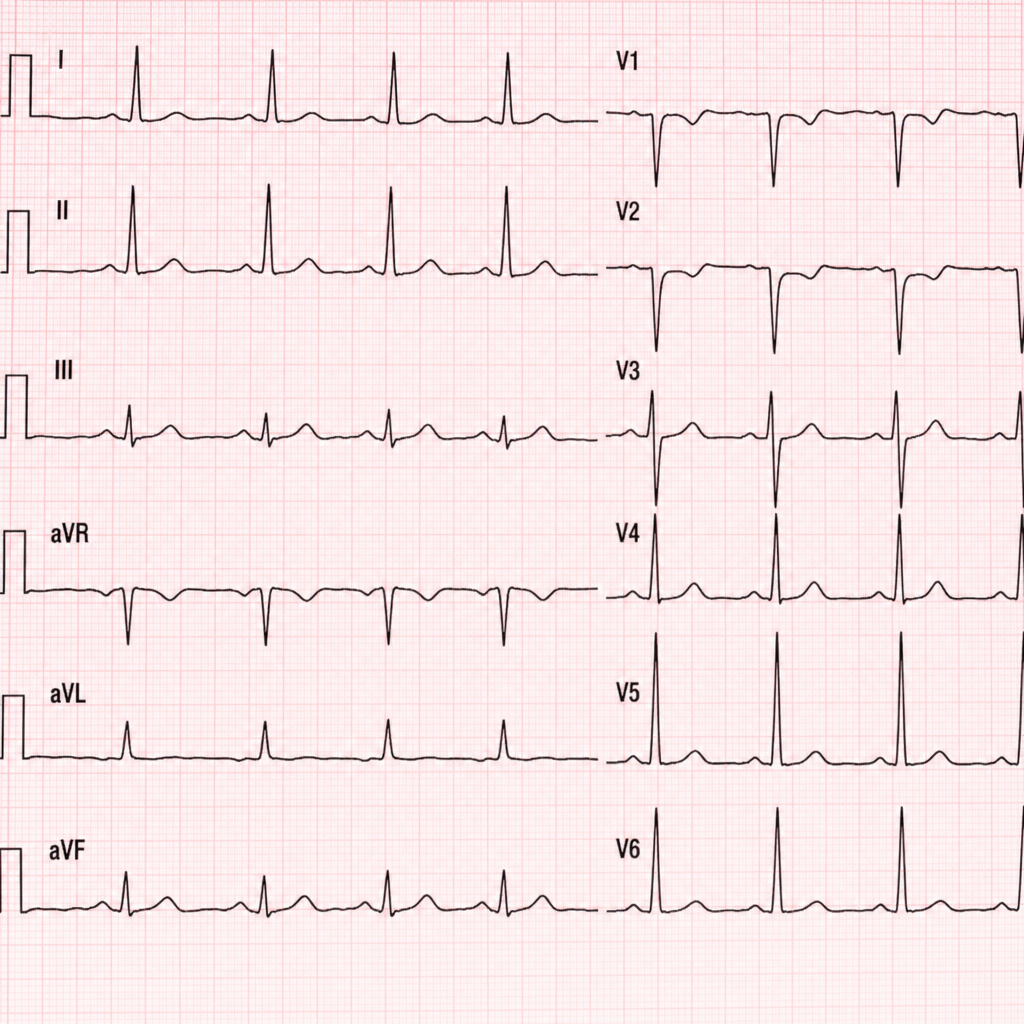
A hypertensive 50-year-old patient presents with diffuse chest pain at rest for 1 hour. CPK-MB is normal and ECG is given below. Which of the following is correct?
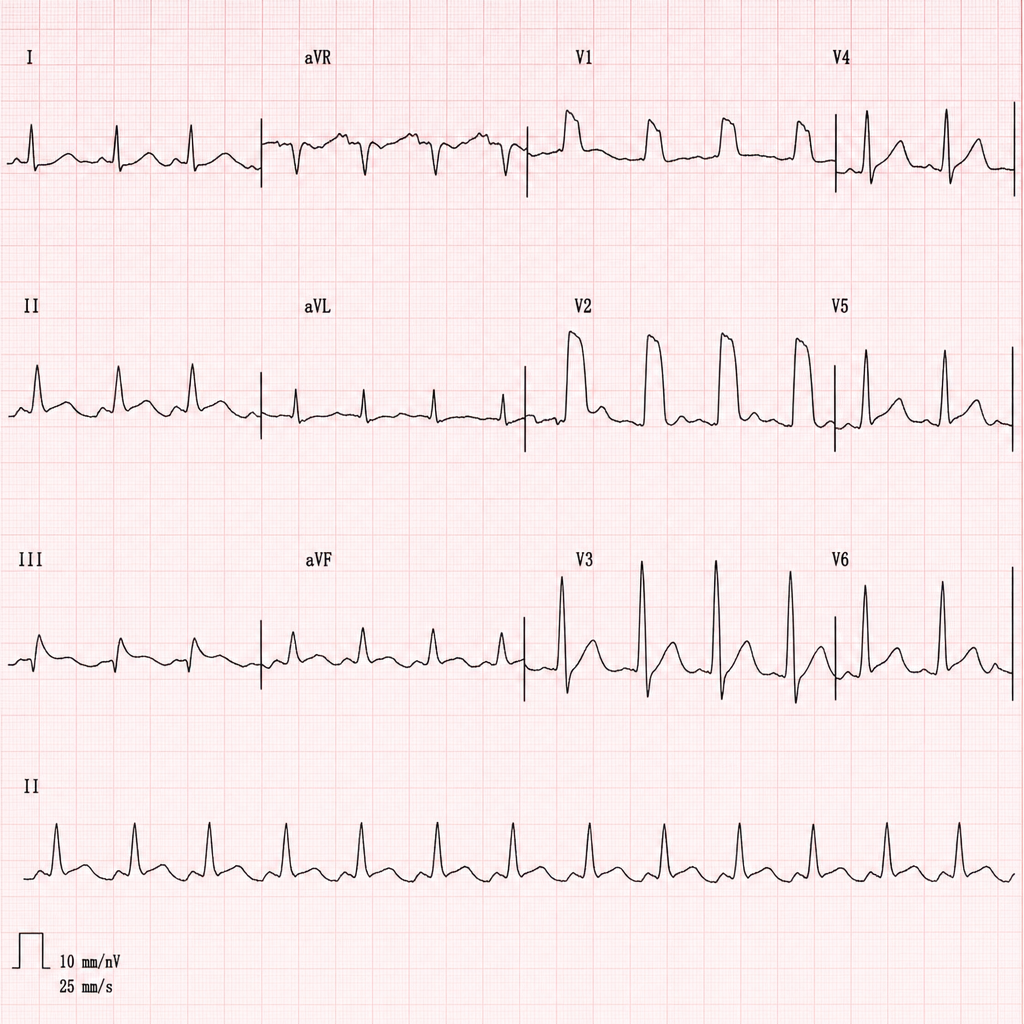
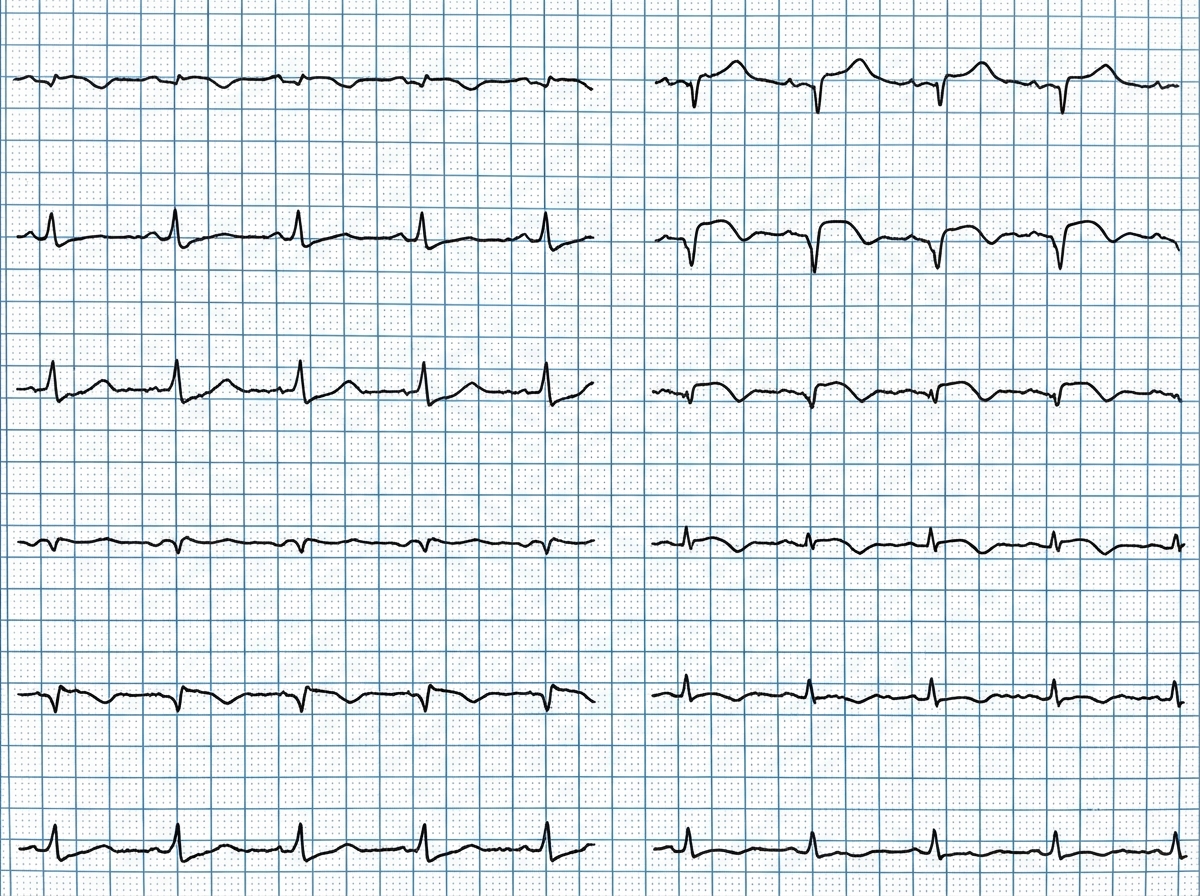
A 65-year-old man is brought with complaints of breathlessness and chest pain for 4 hours. ECG was done. Which of the following is incorrect?
A 65-year-old patient of STEMI underwent thrombolysis with STK. The ECG tracing performed after thrombolysis is shown below. What does it exhibit?
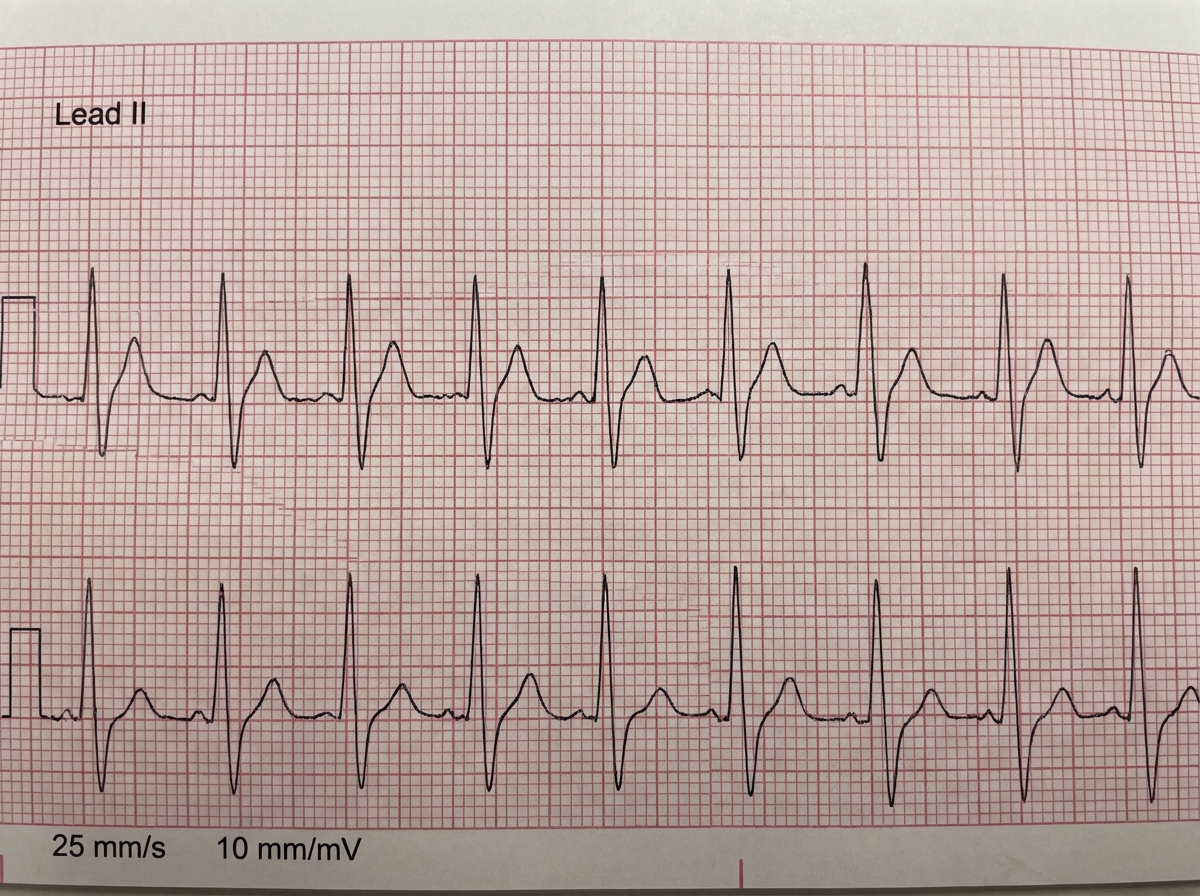
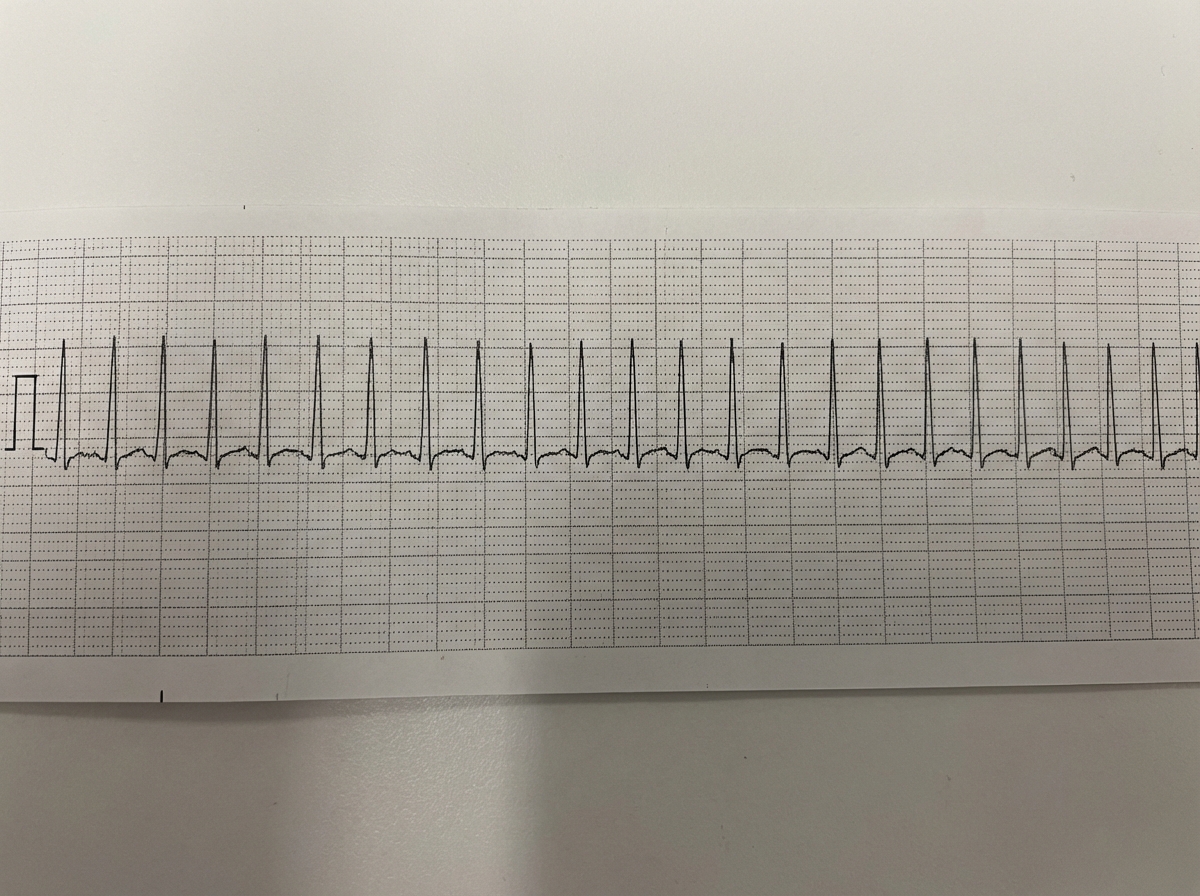
What ECG finding is shown here?
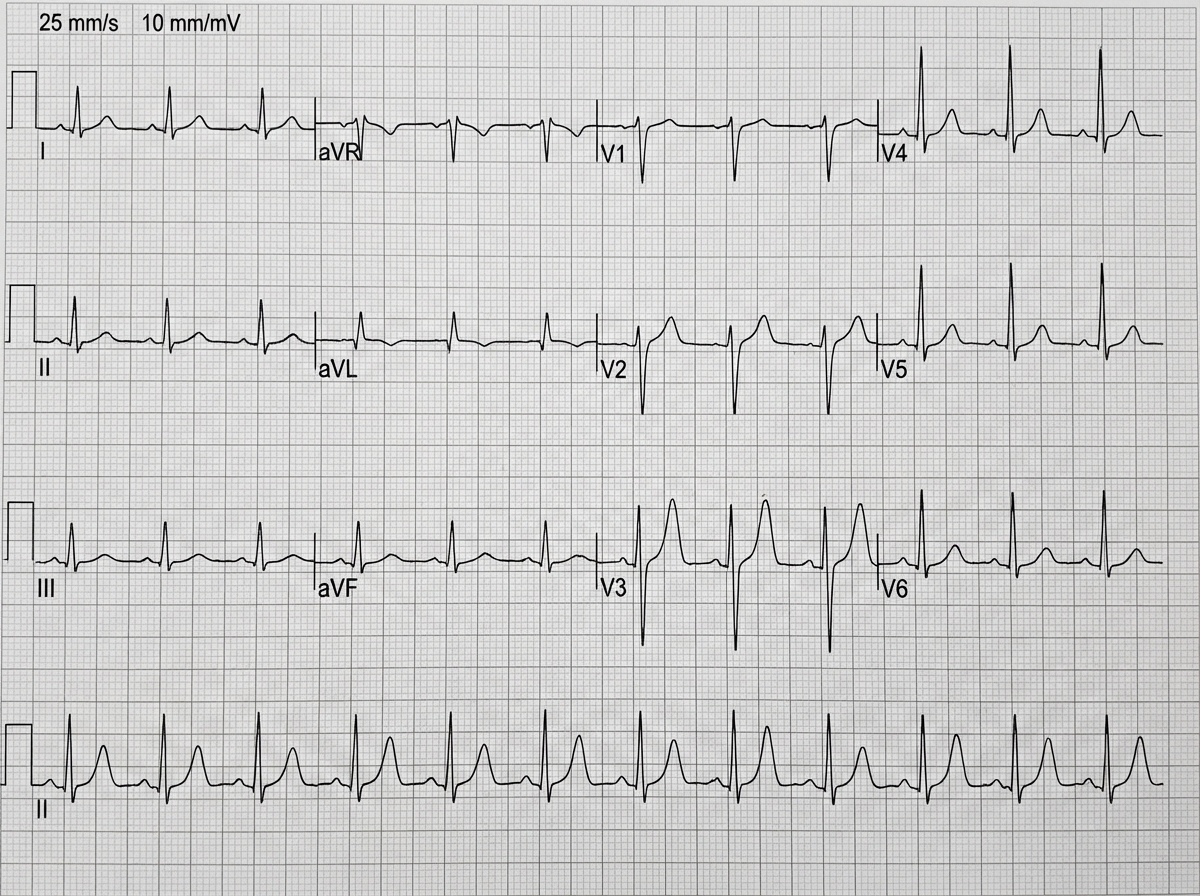
What is incorrect about the ECG shown below?
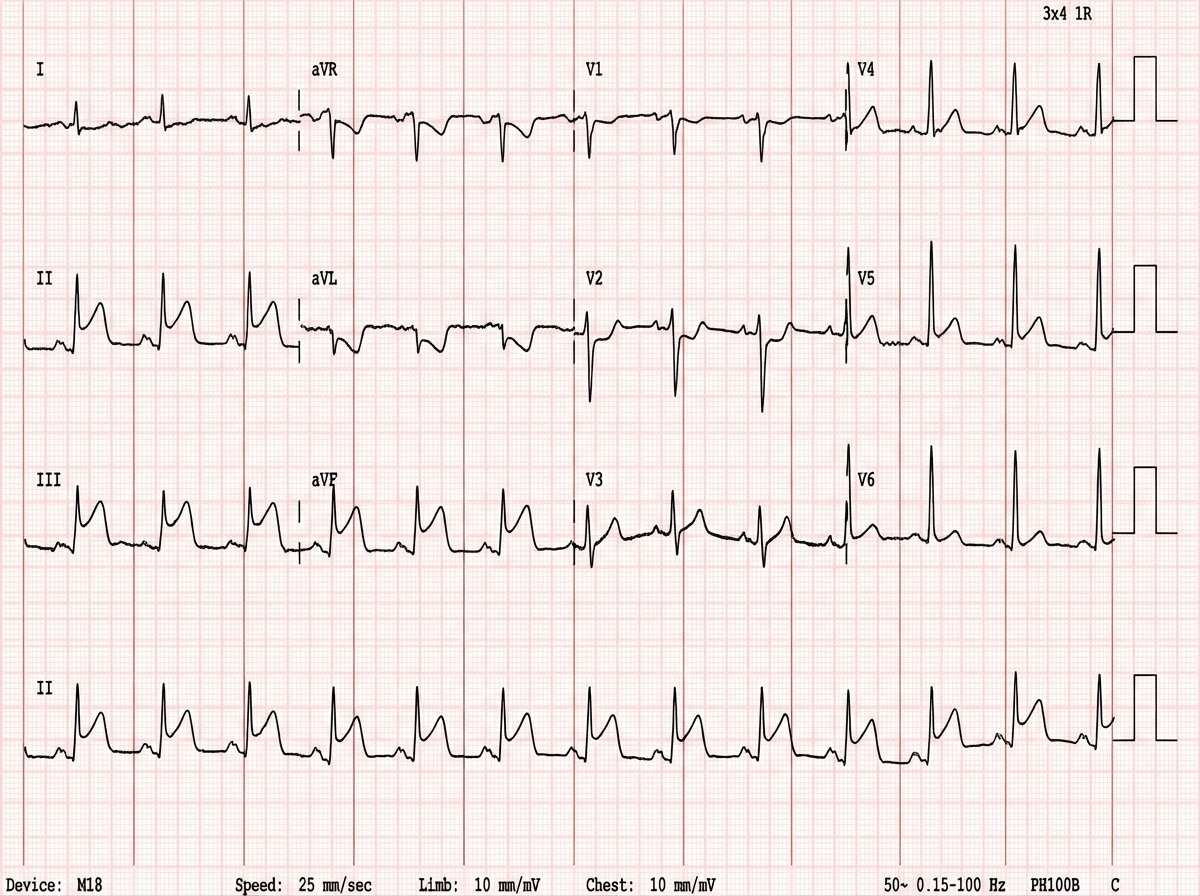
A 50-year-old man is admitted to hospital with Levine sign. BP on admission is 70/50 mm Hg. On auscultation S2 is wide split with S3 gallop rhythm. The ECG is shown below. Which is the correct statement about this patient?
A 40-year-old man was admitted to the hospital emergency with sudden onset of symptoms and signs of severe left ventricular failure. What would be the best management of this patient?
A 50-year-old man is admitted to hospital with Levine sign. BP on admission is 90/60 mm Hg. On auscultation S2 is wide split with S3 gallop rhythm. Which is correct statement about this patient?
Comment on the ECG shown:

A 45-year-old non-smoker presents with increasing breathlessness. The ECG shows:
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app