
Cardiology — MCQs

On this page
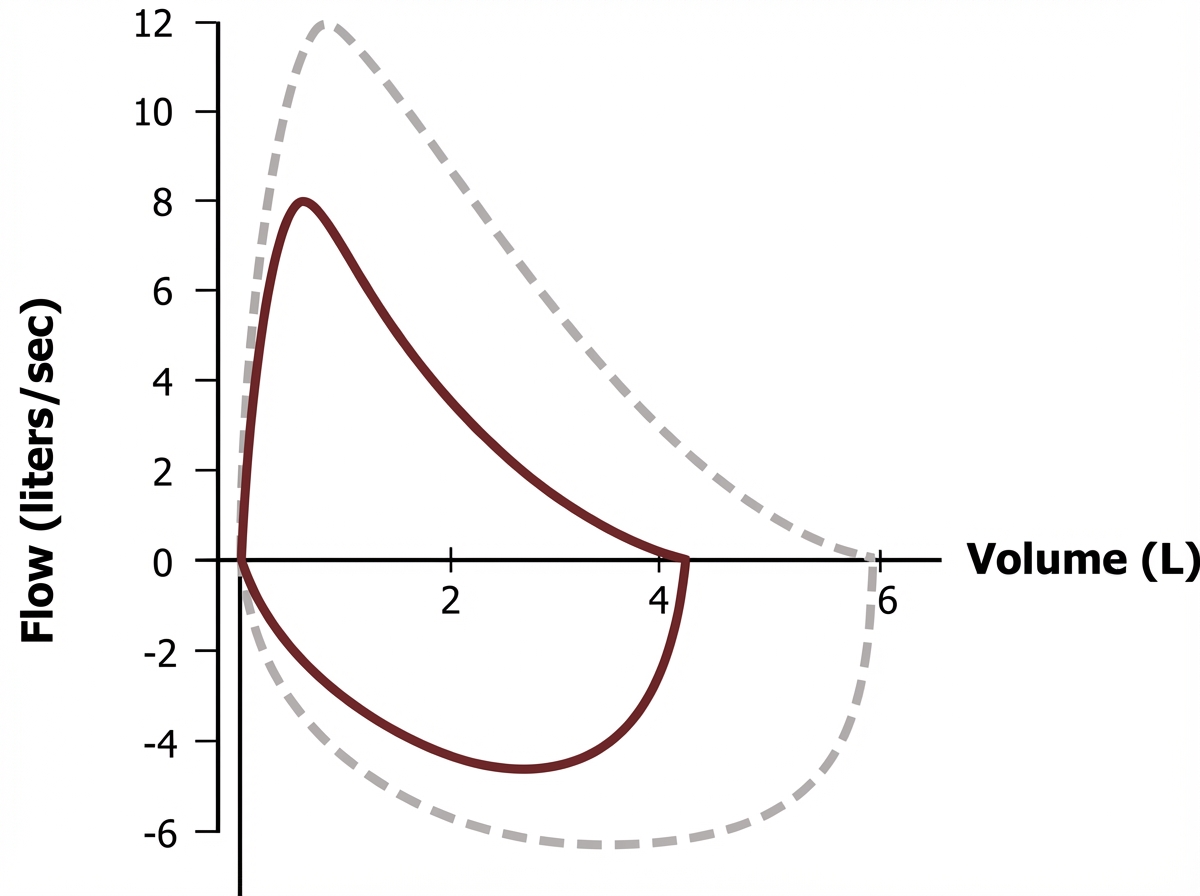
A 47-year-old woman comes to the physician because of a 3-week history of a dry cough. She does not smoke or use illicit drugs. Physical examination shows mild conjunctival hyperemia. Chest auscultation shows fine crackles in both lung fields. Laboratory studies show a total calcium concentration of 10.8 mg/dL. The results of spirometry are shown (dashed loop shows normal for comparison). Further evaluation of this patient is most likely to show an increase in which of the following?
A 77-year-old woman presents to her physician because of fatigue and progressive dyspnea despite receiving optimal treatment for heart failure. Her medical history is positive for heart failure, active tuberculosis, and chronic renal failure, for which she has been in long-term hemodialysis (13 years). The woman currently takes rifampin and isoniazid. Her physical exam shows the presence of hepatomegaly and jugular venous distention that fails to subside on inspiration (Kussmaul's sign) and an impalpable apical impulse. Her pulse is 122/min, respiratory rate 16/min, temperature 36.0°C (97.4°F), and blood pressure 120/60 mm Hg. Her cardiac monitor shows a prominent y descent in her jugular venous pulse. A cardiac ultrasound shows pericardial calcifications and small tubular-shaped ventricles. Which of the following is the most likely cause of this patient's current condition?
A 75-year-old male presents to the emergency room complaining of severe lower abdominal pain and an inability to urinate. He reports that he last urinated approximately nine hours ago. When asked to urinate, only a few drops dribble from the tip of his penis. Further questioning reveals that the patient has experienced progressively worsening difficulty with urinating over the past two years. He has lived alone for five years since his wife passed away. He has not seen a doctor in that time. His temperature is 98.8°F (37.1°C), blood pressure is 145/90 mmHg, pulse is 115/min, and respirations are 22/min. He appears to be in severe pain. Physical examination reveals a distended bladder and significant tenderness to palpation over the inferior aspect of his abdomen. Which of the following sets of lab values would most likely be found in a urinalysis of this patient?
A 27-year-old male presents to the emergency department after being brought in from a house fire. The patient has extensive burns covering his body and is conscious but in severe pain. The patient has a past medical history notable for marijuana use. He is not currently on any medications. Physical exam is notable for extensive burns covering the patient's back, chest, thighs, and legs. The patient's oropharynx reveals no signs of damage or extensive smoke inhalation. The patient is breathing on his own and has normal breath sounds bilaterally. His temperature is 99.5°F (37.5°C), pulse is 145/min, blood pressure is 100/70 mmHg, respirations are 27/min, and oxygen saturation is 93% on room air. Which of the following interventions is most likely to reduce mortality in this patient?
A 69-year-old woman is brought to her primary care physician by her son who is worried about her weight loss. The son reports that over the past 2 months she has lost at least 12 pounds. The patient denies any change in appetite but complains of diarrhea and abdominal discomfort. Additionally, she reports that her stools “smell awful,” which is embarrassing for her. Her son mentions that he feels she is becoming forgetful. She forgets phone conversations and often acts surprised when he visits, even though he always confirms his visits the night before. Her medical history includes arthritis, which she admits has been getting worse, and gastroesophageal reflux disease. She takes omeprazole. She is widowed and recently retired from being a national park ranger. The patient’s temperature is 100.3°F (37.9°C), blood pressure is 107/68 mmHg, and pulse is 88/min. On physical exam, she has a new systolic ejection murmur at the left upper sternal border. Labs show normocytic anemia. A transesophageal echocardiogram reveals a small mobile mass on the aortic valve with moderate aortic insufficiency. A colonoscopy is obtained with a small bowel biopsy. A periodic acid-Schiff stain is positive for foamy macrophages. Which of the following is the best next step in management?
A 75-year-old man presents to his primary care physician for foot pain. The patient states that he has had chronic foot pain, which has finally caused him to come and see the doctor. The patient's past medical history is unknown and he has not seen a doctor in over 50 years. The patient states he has led a healthy lifestyle, consumes a plant-based diet, exercised regularly, and avoided smoking, thus his lack of checkups with a physician. The patient lives alone as his wife died recently. His temperature is 98.1°F (36.7°C), blood pressure is 128/64 mmHg, pulse is 80/min, respirations are 13/min, and oxygen saturation is 98% on room air. The patient's BMI is 19 kg/m^2 and he appears healthy. Physical exam demonstrates a right foot that is diffusely swollen, mildly tender, and deformed. The patient's gait is abnormal. Which of the following is associated with the underlying cause of this patient's presentation?
A 65-year-old woman presents to her primary care physician for a wellness checkup. She states that she has felt well lately and has no concerns. The patient has a 12-pack-year smoking history and has 3 drinks per week. She is retired and lives at home with her husband. She had a normal colonoscopy 8 years ago and mammography 1 year ago. She can't recall when she last had a Pap smear and believes that it was when she was 62 years of age. Her temperature is 98.1°F (36.7°C), blood pressure is 137/78 mmHg, pulse is 80/min, respirations are 13/min, and oxygen saturation is 98% on room air. Physical exam is within normal limits. Which of the following is the best next step in management?
A 23-year-old woman comes to the physician because of increasing pain and swelling of her hands and wrists for 3 days. She has been unable to continue her daily activities like writing or driving. She has had a nonpruritic generalized rash for 4 days. She had fever and a runny nose one week ago which resolved with over-the-counter medication. She is sexually active with a male partner and uses condoms inconsistently. She works as an attendant at an amusement park. Her temperature is 37.1°C (98.8°F), pulse is 90/min, and blood pressure is 118/72 mm Hg. Examination shows swelling and tenderness of the wrists as well as the metacarpophalangeal and proximal interphalangeal joints. Range of motion at the wrists is limited. A lacy macular rash is noted over the trunk and extremities. The remainder of the examination shows no abnormalities. Laboratory studies, including erythrocyte sedimentation rate and anti-nuclear antibody and anti-dsDNA serology, show no abnormalities. Which of the following is the most likely diagnosis?
A 70-year-old woman is evaluated for muscle pain and neck stiffness that has been progressing for the past 3 weeks. She reports that the neck stiffness is worse in the morning and gradually improves throughout the day. She feels fatigued, although there have not been any changes in her daily routine. Her past medical history includes coronary artery disease for which she takes a daily aspirin. Both of her parents died in their 80s from cardiovascular disease. Her blood pressure is 140/90 mm Hg, heart rate is 88/min, respiratory rate is 15/min, and temperature is 37.9°C (100.2°F). On further examination, the patient has difficulty standing up from a seated position, although muscle strength is intact. What is the best next step in management?
A 21-year-old man presents to his physician because he has been feeling increasingly tired and short of breath at work. He has previously had these symptoms but cannot recall the diagnosis he was given. Chart review reveals the following results: Oxygen tension in inspired air = 150 mmHg Alveolar carbon dioxide tension = 50 mmHg Arterial oxygen tension = 71 mmHg Respiratory exchange ratio = 0.80 Diffusion studies reveal normal diffusion distance. The patient is administered 100% oxygen but the patient's blood oxygen concentration does not improve. Which of the following conditions would best explain this patient's findings?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app