
Cardiology — MCQs

On this page
A 70-year-old woman presents to her primary care doctor complaining of left knee pain. She states that she has noticed this more during the past several months after a fall at home. Previously, she was without pain and has no history of trauma to her knees. The patient states that the majority of her pain starts in the afternoon after she has been active for some time, and that the pain resolves with rest and over-the-counter analgesics. Aside from the left knee, she has no other symptoms and no other joint findings. On exam, her temperature is 98.8°F (37.1°C), blood pressure is 124/76 mmHg, pulse is 70/min, and respirations are 12/min. The patient has no limitations in her range of motion and no changes in strength on motor testing. However, there is tenderness along the medial joint line. What finding is most likely seen in this patient?
A 57-year-old woman is brought to the emergency department by her husband with complaints of sudden-onset slurring for the past hour. She is also having difficulty holding things with her right hand. She denies fever, head trauma, diplopia, vertigo, walking difficulties, nausea, and vomiting. Past medical history is significant for type 2 diabetes mellitus, hypertension, and hypercholesterolemia for which she takes a baby aspirin, metformin, ramipril, and simvastatin. She has a 23-pack-year cigarette smoking history. Her blood pressure is 148/96 mm Hg, the heart rate is 84/min, and the temperature is 37.1°C (98.8°F). On physical examination, extraocular movements are intact. The patient is dysarthric, but her higher mental functions are intact. There is a right-sided facial weakness with preserved forehead wrinkling. Her gag reflex is weak. Muscle strength is mildly reduced in the right hand. She has difficulty performing skilled movements with her right hand, especially writing, and has difficulty touching far objects with her index finger. She is able to walk without difficulty. Pinprick and proprioception sensation is intact. A head CT scan is within normal limits. What is the most likely diagnosis?
A 56-year-old man comes to the physician because of worsening double vision and drooping of the right eyelid for 2 days. He has also had frequent headaches over the past month. Physical examination shows right eye deviation laterally and inferiorly at rest. The right pupil is dilated and does not react to light or with accommodation. The patient's diplopia improves slightly on looking to the right. Which of the following is the most likely cause of this patient’s findings?
A 76-year-old female with a past medical history of obesity, coronary artery disease status post stent placement, hypertension, hyperlipidemia, and insulin dependent diabetes comes to your outpatient clinic for regular checkup. She has not been very adherent to her diabetes treatment regimen. She has not been checking her sugars regularly and frequently forgets to administer her mealtime insulin. Her Hemoglobin A1c three months ago was 14.1%. As a result of her diabetes, she has developed worsening diabetic retinopathy and neuropathy. Based on her clinical presentation, which of the following is the patient most at risk for developing?
A 37-year-old-man presents to the clinic for a 2-month follow-up. He is relatively healthy except for a 5-year history of hypertension. He is currently on lisinopril, amlodipine, and hydrochlorothiazide. The patient has no concerns and denies headaches, weight changes, fever, chest pain, palpitations, vision changes, or abdominal pain. His temperature is 98.9°F (37.2°C), blood pressure is 157/108 mmHg, pulse is 87/min, respirations are 15/min, and oxygen saturation is 98% on room air. Laboratory testing demonstrates elevated plasma aldosterone concentration and low renin concentration. What is the most likely explanation for this patient’s presentation?
Please refer to the summary above to answer this question. Further evaluation of this patient is most likely to show which of the following findings? Patient Information Age: 28 years Gender: F, self-identified Ethnicity: unspecified Site of Care: office History Reason for Visit/Chief Concern: "I'm not making breast milk anymore." History of Present Illness: 1-week history of failure to lactate; has previously been able to breastfeed her twins, who were born 12 months ago menses resumed 4 months ago but have been infrequent feels generally weak and tired has had a 6.8-kg (15-lb) weight gain over the past 2 months despite having a decreased appetite Past Medical History: vaginal delivery of twins 12 months ago, complicated by severe postpartum hemorrhage requiring multiple blood transfusions atopic dermatitis Social History: does not smoke, drink alcohol, or use illicit drugs is not sexually active Medications: topical triamcinolone, multivitamin Allergies: no known drug allergies Physical Examination Temp Pulse Resp BP O2 Sat Ht Wt BMI 37°C (98.6°F) 54/min 16/min 101/57 mm Hg – 160 cm (5 ft 3 in) 70 kg (154 lb) 27 kg/m2 Appearance: tired-appearing HEENT: soft, nontender thyroid gland without nodularity Pulmonary: clear to auscultation Cardiac: bradycardic but regular rhythm; normal S1 and S2; no murmurs, rubs, or gallops Breast: no nodules, masses, or tenderness; no nipple discharge Abdominal: overweight; no tenderness, guarding, masses, bruits, or hepatosplenomegaly; normal bowel sounds Extremities: mild edema of the ankles bilaterally Skin: diffusely dry Neurologic: alert and oriented; cranial nerves grossly intact; no focal neurologic deficits; prolonged relaxation phase of multiple deep tendon reflexes
A 59-year-old man presents to his primary care physician complaining of leg pain with exertion for the last 6 months. He has cramping in his calves when walking. He states that the cramping is worse on the right than the left and that the cramping resolves when he stops walking. He has had type 2 diabetes mellitus for 15 years and is not compliant with his medications. He has smoked 20–30 cigarettes daily for the past 30 years. On examination, the femoral pulses are diminished on both sides. Which of the following is the most likely cause of this patient’s condition?
A 55-year-old man comes to the physician for a follow-up examination. For the past 6 months, he has had fatigue, headaches, and several episodes of dizziness. Three months ago, he was diagnosed with hypertension and started on medications. Since the diagnosis was made, his medications have been adjusted several times because of persistently high blood pressure readings. He also has hypercholesterolemia and peripheral arterial disease. He smoked one pack of cigarettes daily for 34 years but quit two months ago. His current medications include aspirin, atorvastatin, losartan, felodipine, and hydrochlorothiazide. He is 188 cm (6 ft 2 in) tall and weighs 109 kg (240 lb); BMI is 31 kg/m2. His pulse is 82/min and blood pressure is 158/98 mm Hg. Physical examination shows bilateral carotid bruits and normal heart sounds. Serum potassium concentration is 3.2 mEq/L, plasma renin activity is 4.5 ng/mL/h (N = 0.3–4.2 ng/mL/h), and serum creatinine concentration is 1.5 mg/dL. Further evaluation of this patient is most likely to show which of the following findings?
A 45-year-old male is presenting for routine health maintenance. He has no complaints. His pulse is 75/min, blood pressure is 155/90 mm Hg, and respiratory rate is 15/min. His body mass index is 25 kg/m2. The physical exam is within normal limits. He denies any shortness of breath, daytime sleepiness, headaches, sweating, or palpitations. He does not recall having an elevated blood pressure measurement before. Which of the following is the best next step?
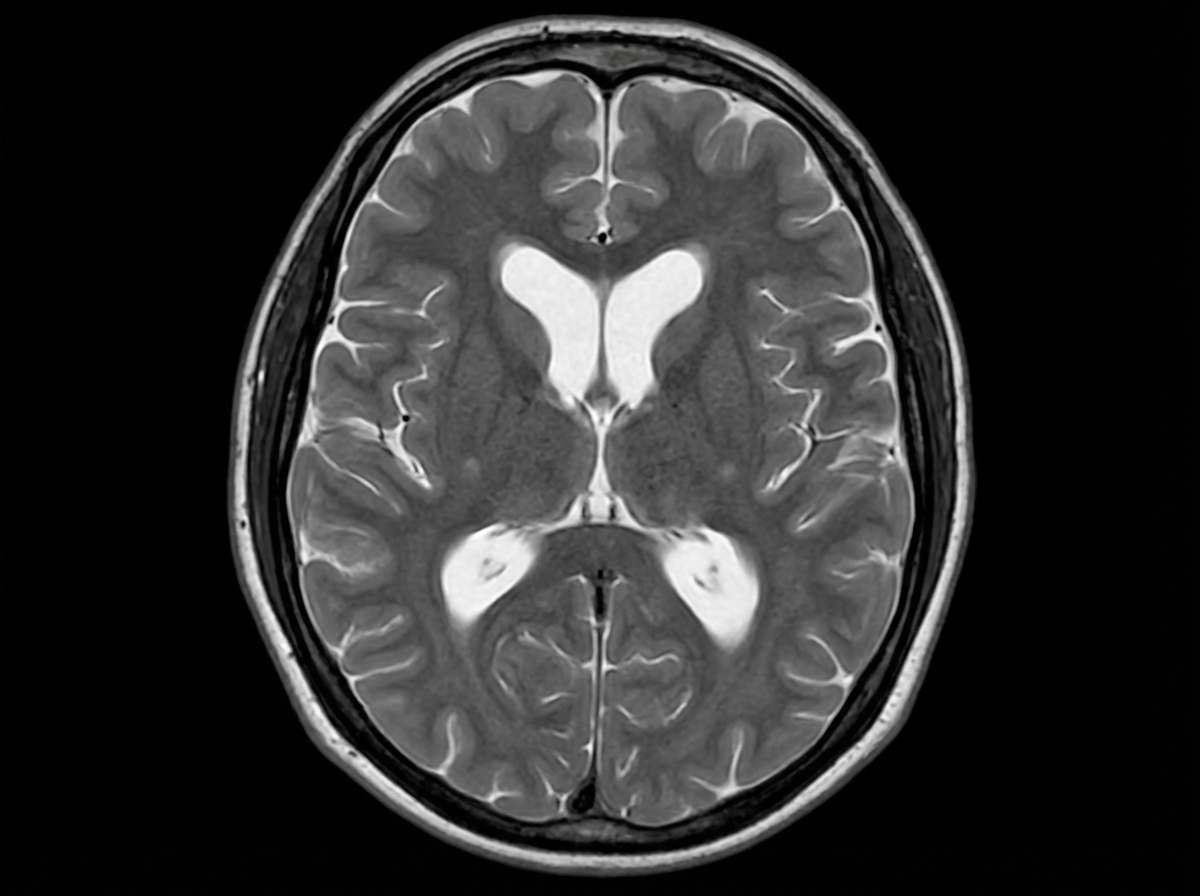
A 74-year-old man is brought to the physician by his wife for progressively worsening confusion and forgetfulness. Vital signs are within normal limits. Physical examination shows a flat affect and impaired short-term memory. An MRI of the brain is shown. Further evaluation of this patient is most likely to show which of the following findings?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app