
Cardiology — MCQs

On this page
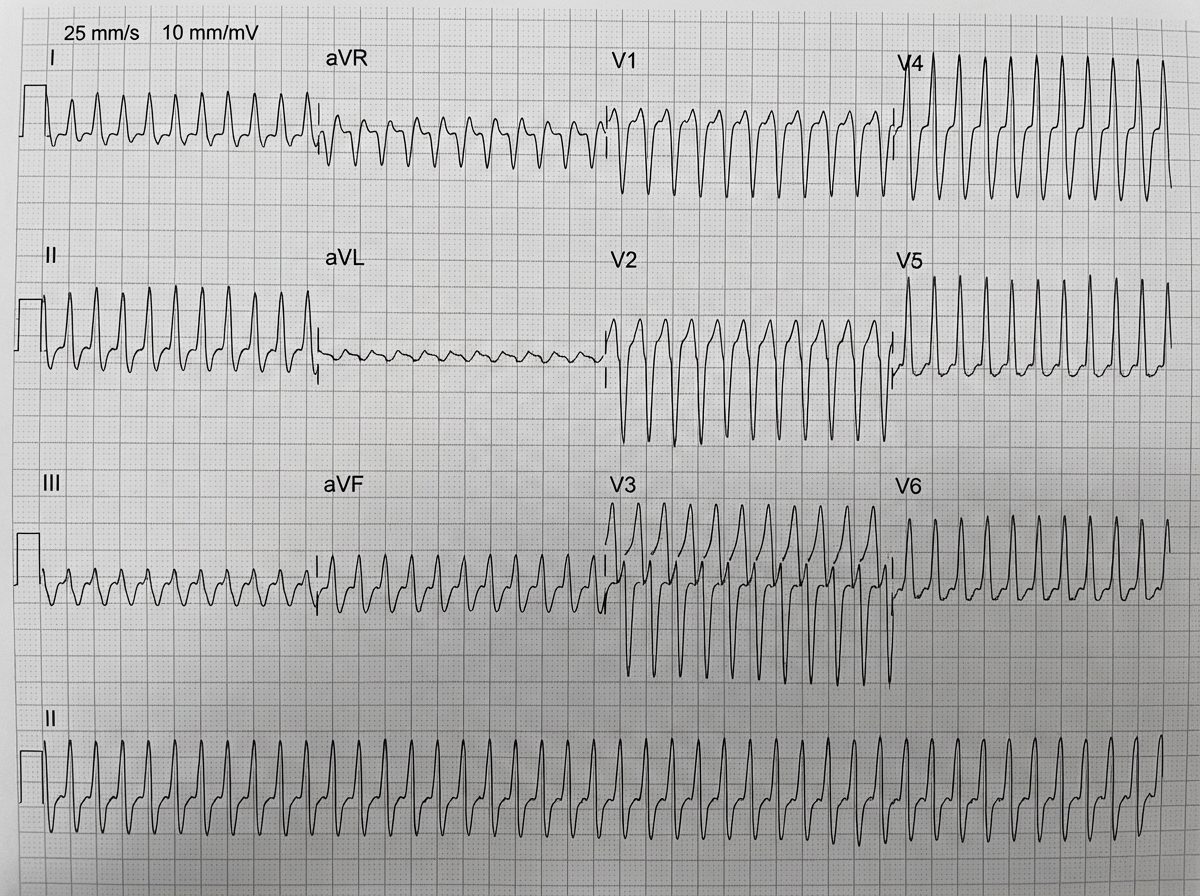
A hemodynamically stable patient presents with the ECG shown below, demonstrating a regular monomorphic wide-complex tachycardia of uncertain origin (ventricular tachycardia vs. SVT with aberrancy). Which of the following drugs is contraindicated in this setting?
What does the following ECG show?
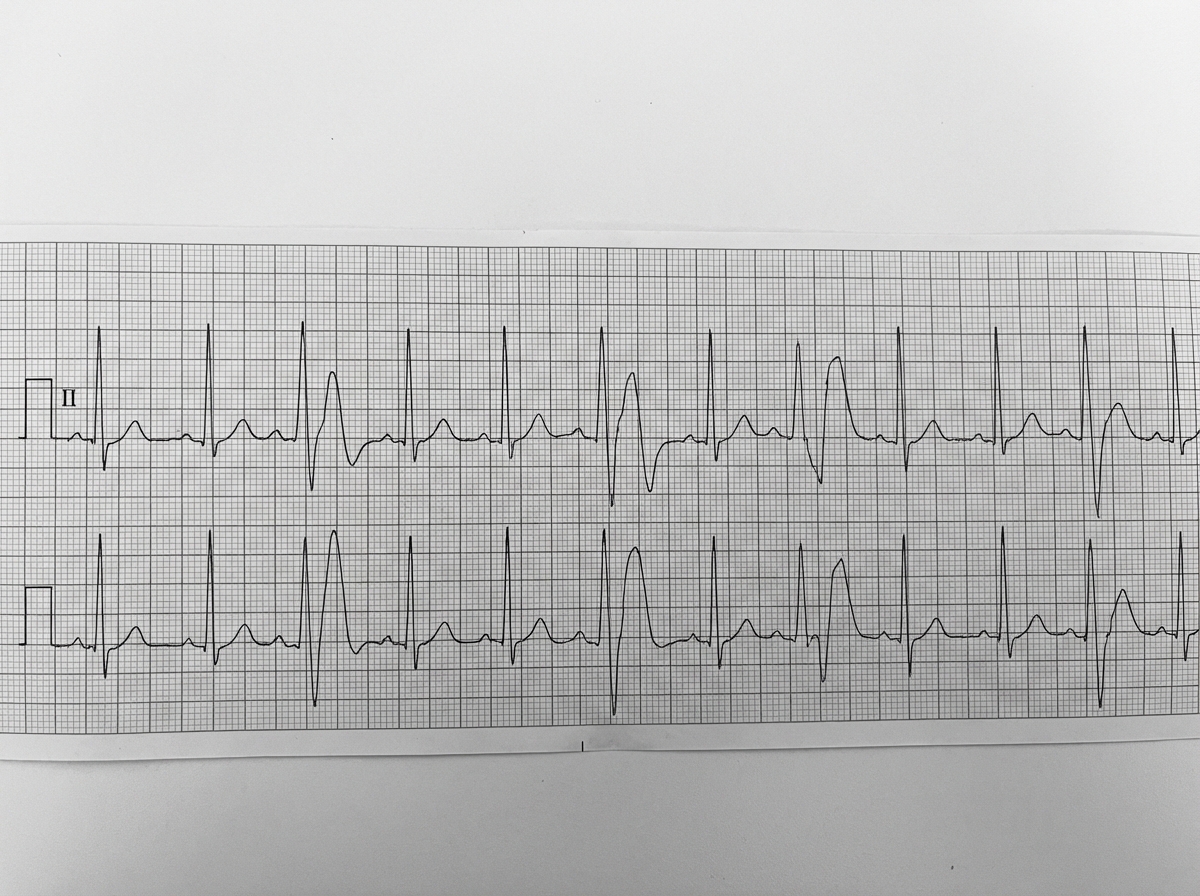
Comment on the ECG findings.
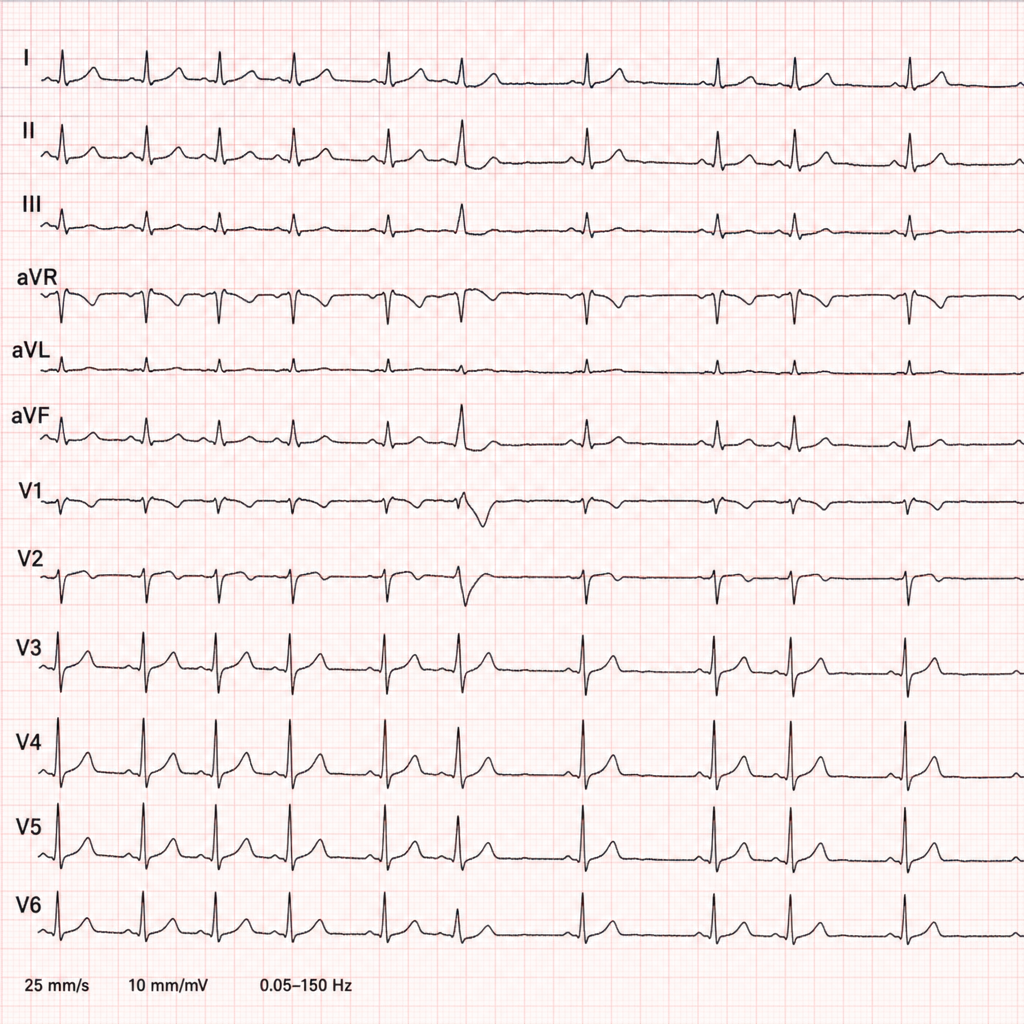
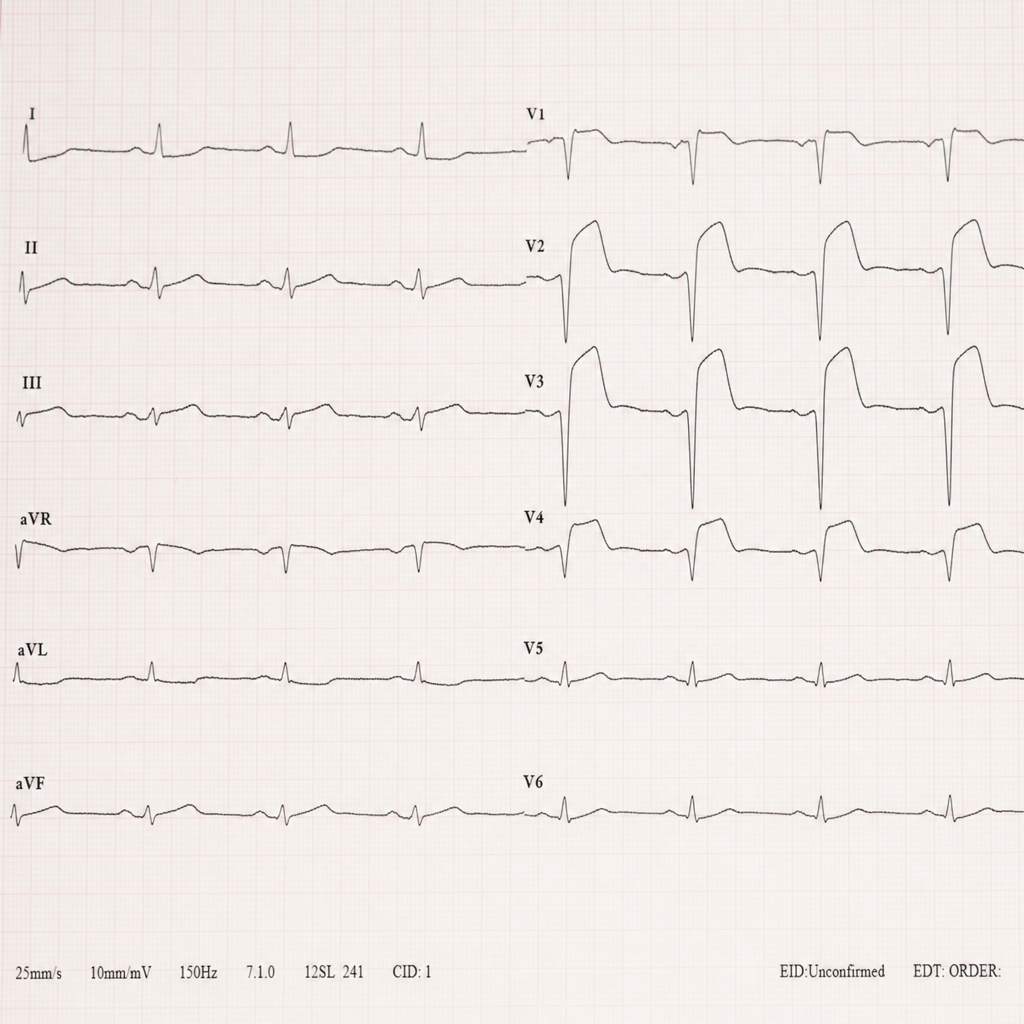
A 35-year-old lady has been diagnosed with anxiety neurosis by her psychiatrist. She came to you for second opinion. Comment on the diagnosis based on ECG.
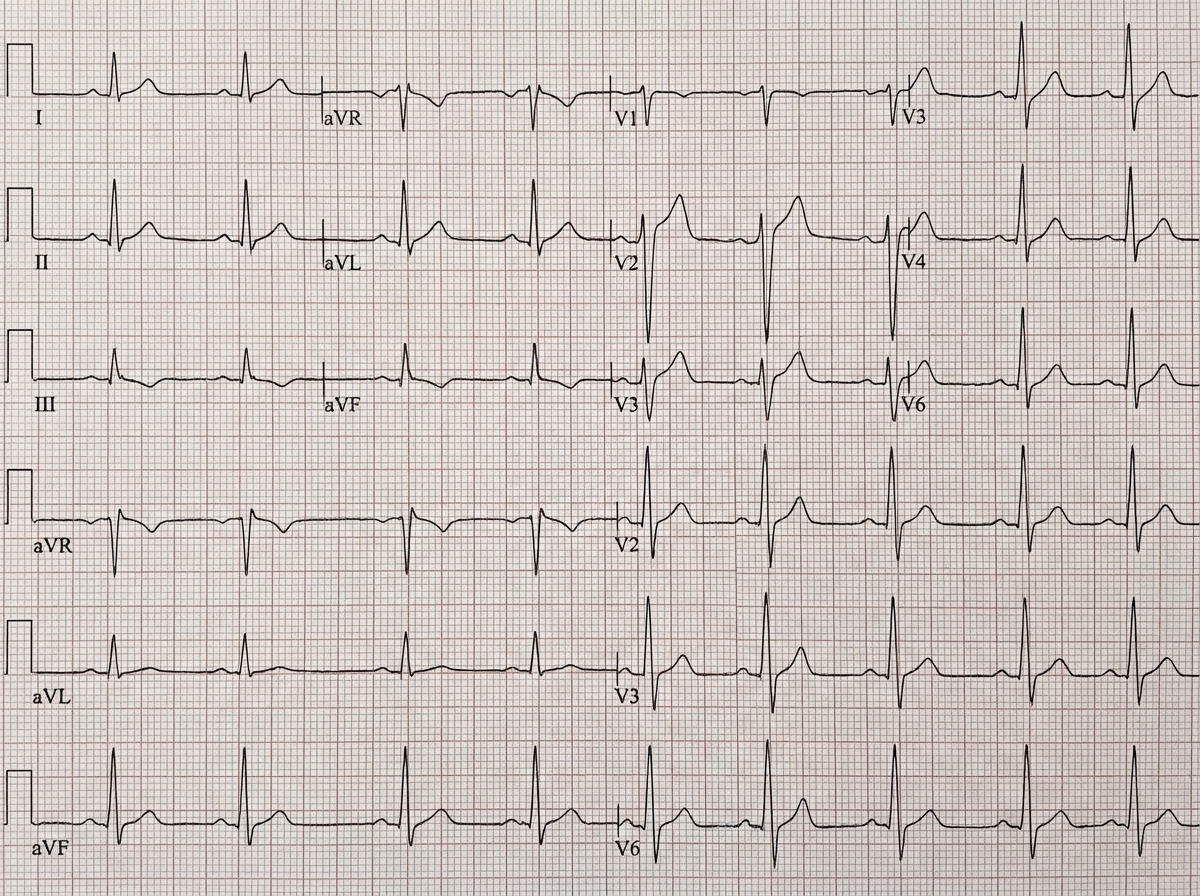
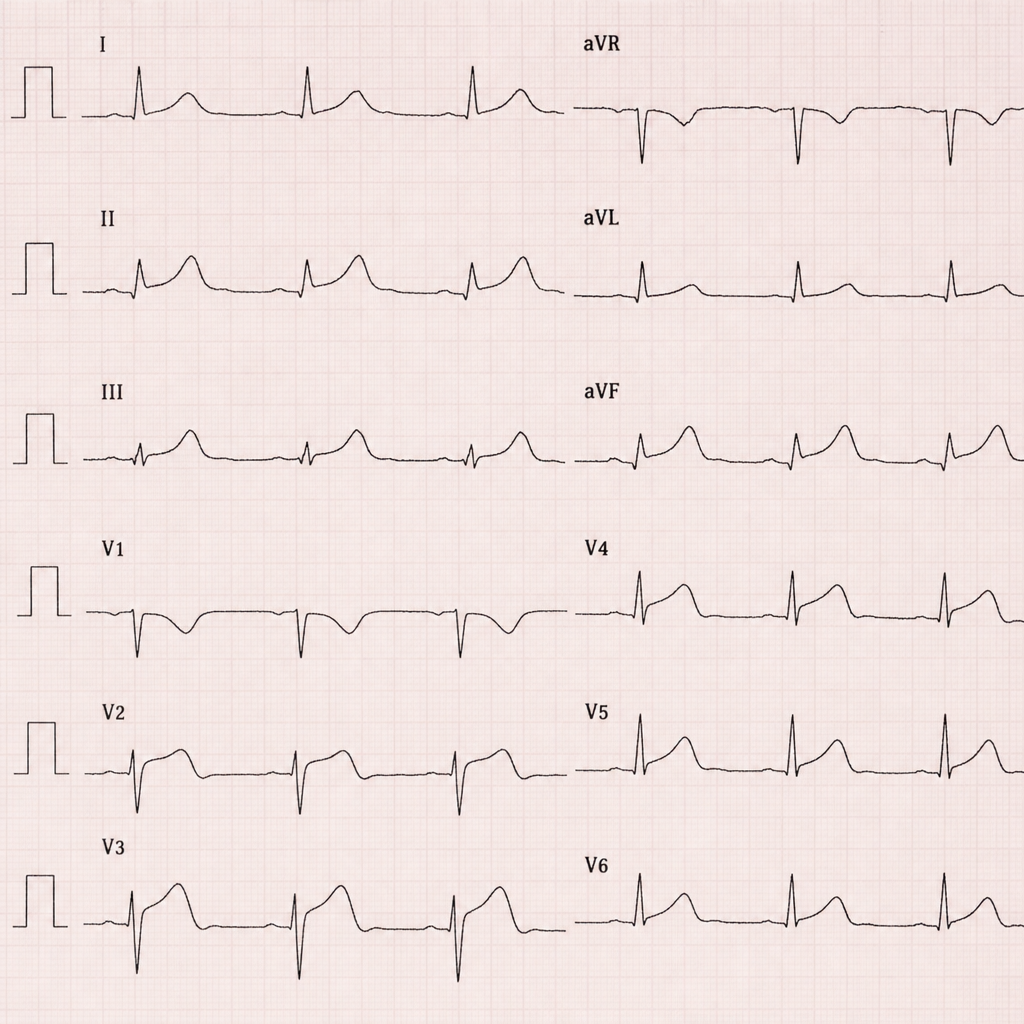
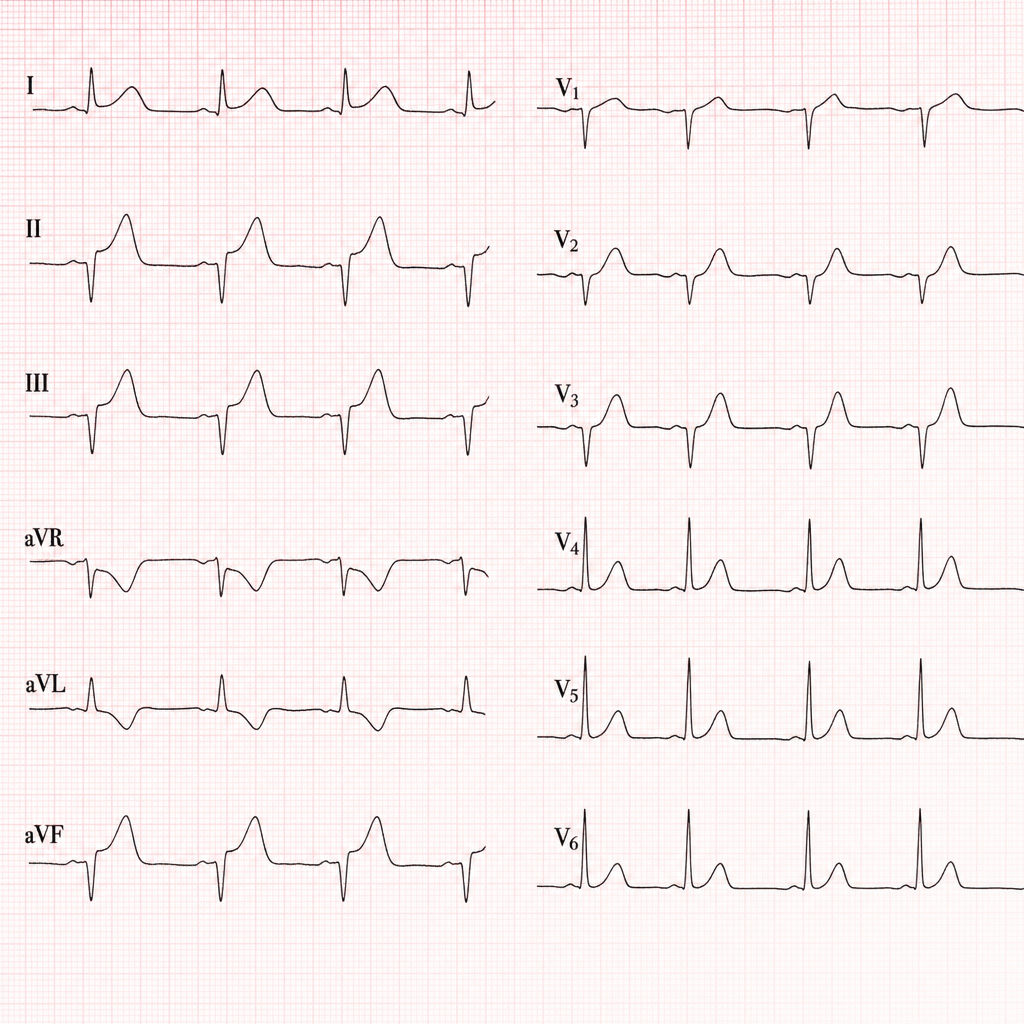
A 46-year-old man presents with diffuse chest pain at rest and recent history of cough, fever and rhinorrhea lasting for 3 days. ECG shows diffuse ST-segment elevation with PR-segment depression. What is the most likely diagnosis?
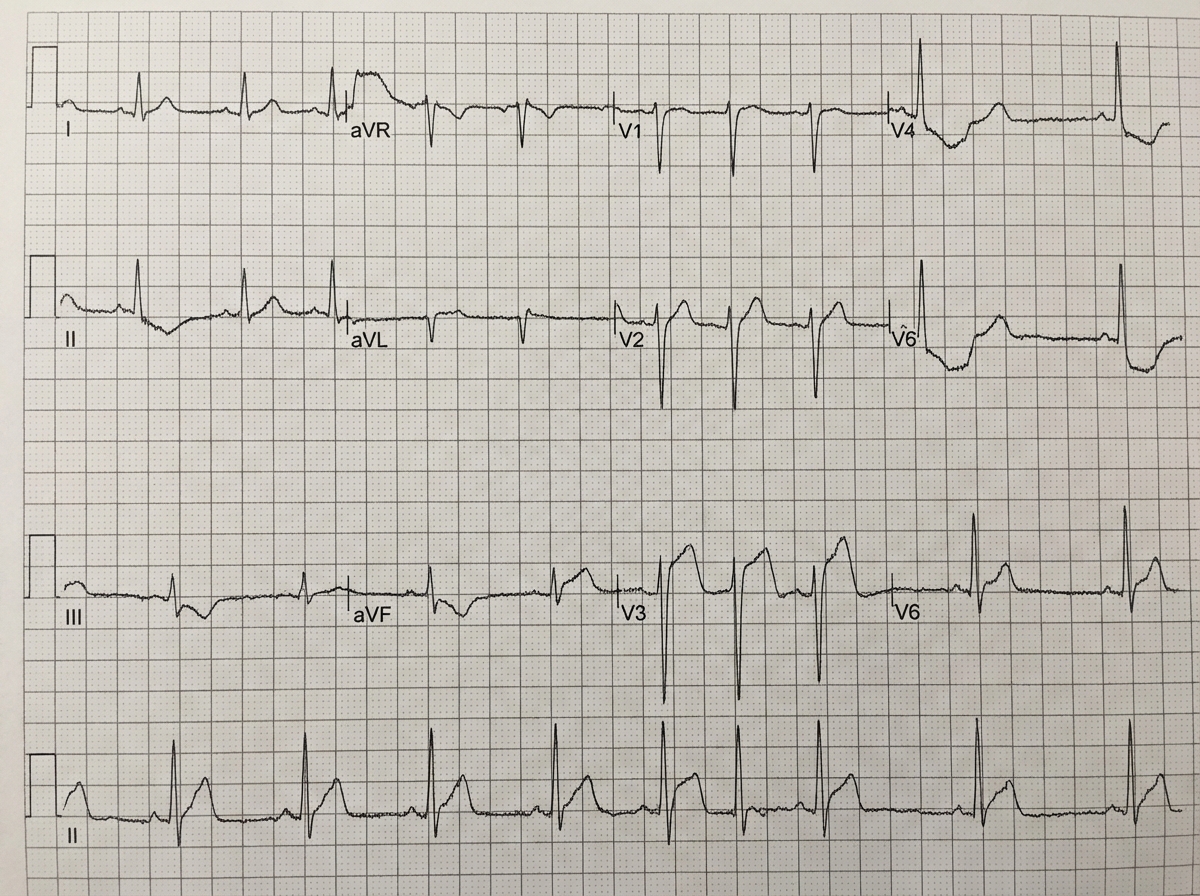
A 70-year-old hypertensive woman presents with dyspnea, nausea and feeling of impending doom. Serial ECGs show persistent ST-segment elevations and troponin levels are elevated. ECG shows:
Comment on the ECG given below:
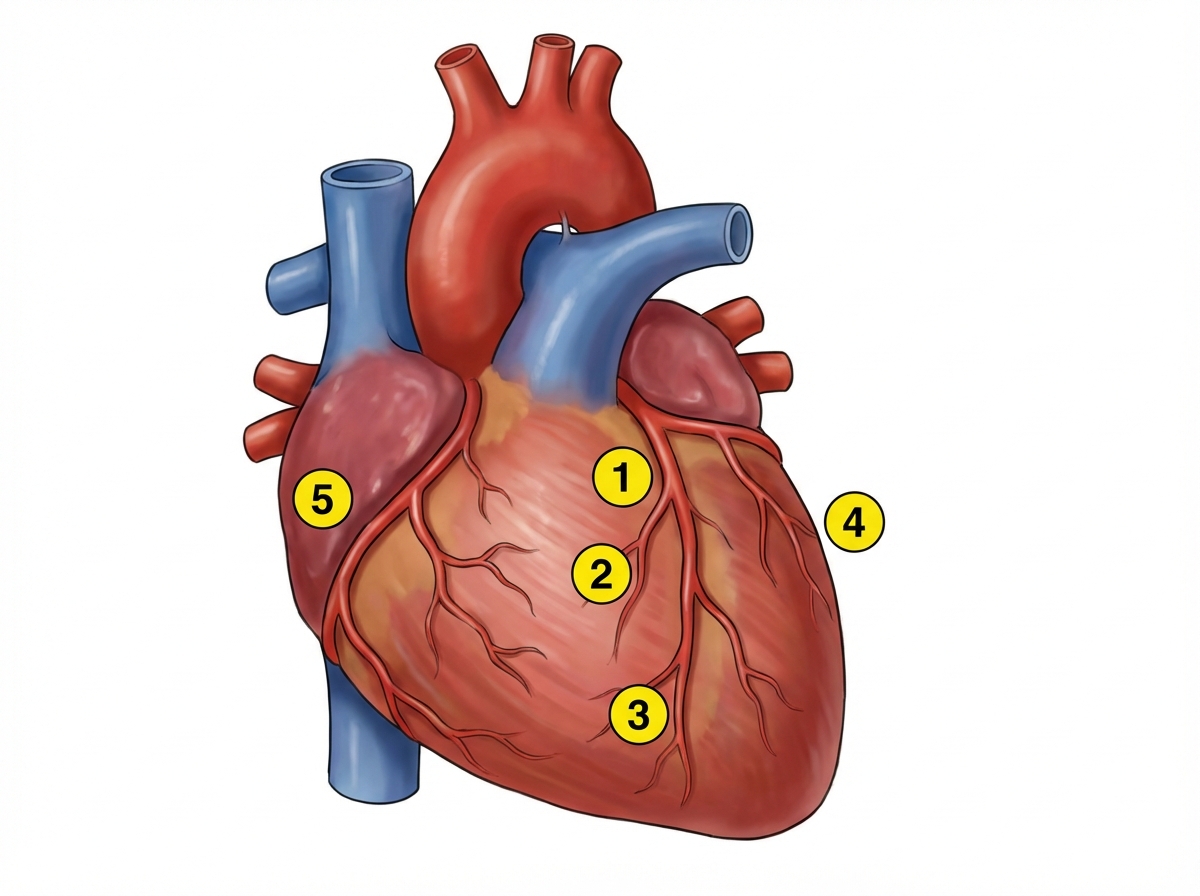
ECG of a patient had ST segment elevation in V1-V6, lead I and AVL. Which of the following branches is involved?
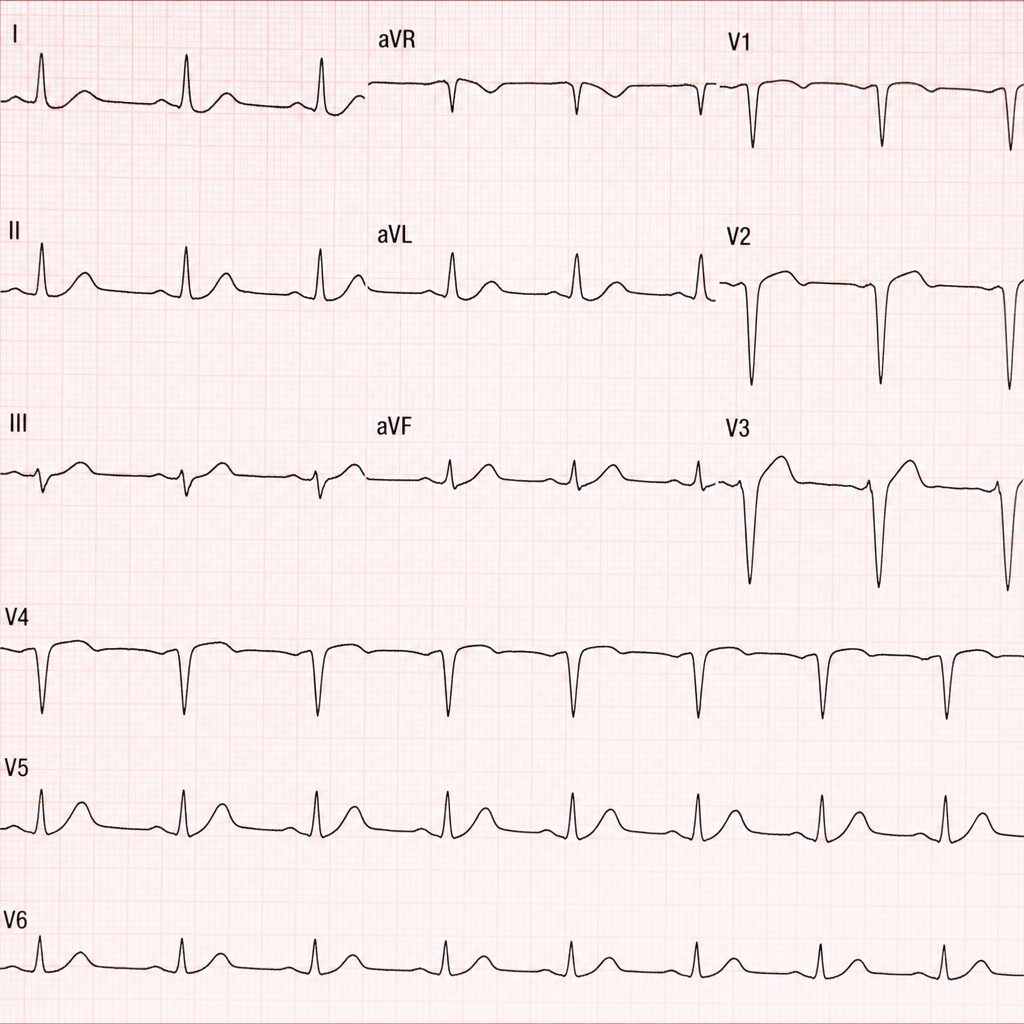
A 65-year-old diabetic lady complains of bloating for 3 hours. What is the diagnosis?
A patient collapsed while waiting for boarding an aircraft and was rushed to the medical room. Which of the following is correct regarding the ECG?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app