
Cardiology — MCQs

On this page
A 34-year-old G3P3 woman with a history of migraines presents with several weeks of headaches. The headaches are unlike her usual migraines and are worse in the morning. This morning she had an episode of emesis prompting her to seek medical care. She also has some right sided weakness which she believes is related to a new exercise routine. Her mother is a breast cancer survivor. Her medications include oral contraceptives and ibuprofen as needed, which has not helped her current headaches. She drinks 2-3 alcoholic drinks on the weekends and does not smoke. Physical examination is remarkable for bilateral papilledema. Motor exam is notable for upper and lower extremity strength 4/5 on the right and 5/5 on the left. Magnetic resonance venography demonstrates absent flow in the left venous sinuses. Which of the following predisposed this patient to her current condition?
A 52-year-old man presents to the emergency department with sudden-onset dyspnea, tachypnea, and chest pain. He works as a long-haul truck driver, and he informs you that he recently returned to the west coast from a trip to Tennessee. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type 2, and mild intellectual disability. He currently smokes 2 packs of cigarettes/day, drinks a 6-pack of beer/day, and he endorses a past history of injection drug use but currently denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 23/min. His physical examination shows minimal bibasilar rales, but otherwise clear lungs on auscultation, grade 2/6 holosystolic murmur, and a benign abdominal physical examination. A computed tomography angiography (CTA) demonstrates a segmental pulmonary embolism (PE). Which of the following is the most appropriate treatment plan for this patient?
A 65-year-old male engineer presents to the office with shortness of breath on exertion and a dry cough that he has had for about a year. He is a heavy smoker with a 25-pack-years history. His vitals include: heart rate 95/min, respiratory rate 26/min, and blood pressure 110/75 mm Hg. On examination, he presents with nail clubbing and bilateral and persistent crackling rales. The chest radiograph shows basal reticulonodular symmetric images, with decreased lung fields. The pulmonary function tests show the following: diffusing capacity of the lungs for carbon monoxide (DLCO) is 43% and reference SaO2 is 94% and 72%, at rest and with exercise, respectively. What is the most likely diagnosis?
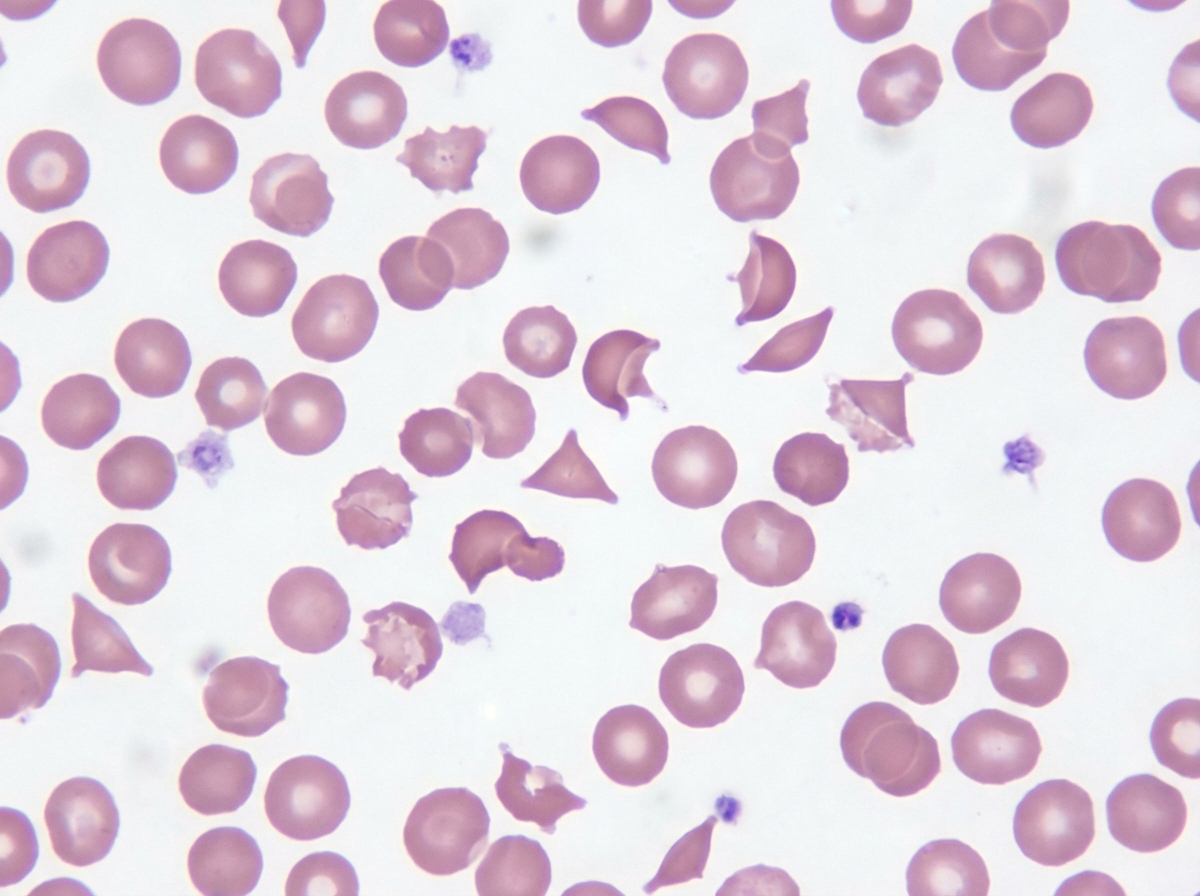
A 62-year-old man presents to his primary care physician because he has noticed his skin and eyes have been turning yellow. He has no other complaints except that he has been getting tired more easily, which he attributes to normal aging. Based on clinical suspicion a panel of tests are performed with the following results: Hemoglobin: 11 g/dL Leukocyte count: 5,370/mm^3 Platelet count: 168,000/mm^3 Mean corpuscular volume: 95 µm^3 Haptoglobin level: Decreased Reticulocytes: 3% Peripheral blood smear is also obtained and shown in the figure provided. Which of the following patient characteristics is consistent with the most likely cause of this patient's disease?
A 51-year-old woman is brought into the emergency department following a motor vehicle accident. She is unconscious and was intubated in the field. Past medical history is unknown. Upon arrival, she is hypotensive and tachycardic. Her temperature is 37.2°C (99.1°F), the pulse is 110/min, the respiratory rate is 22/min, and the blood pressure is 85/60 mm Hg. There is no evidence of head trauma, she withdraws to pain and her pupils are 2mm and reactive to light. Her heart has a regular rhythm without any murmurs or rubs and her lungs are clear to auscultation. Her abdomen is firm and distended with decreased bowel sounds. Her extremities are cool and clammy with weak, thready pulses. There is no peripheral edema. Of the following, what is the likely cause of her presentation?
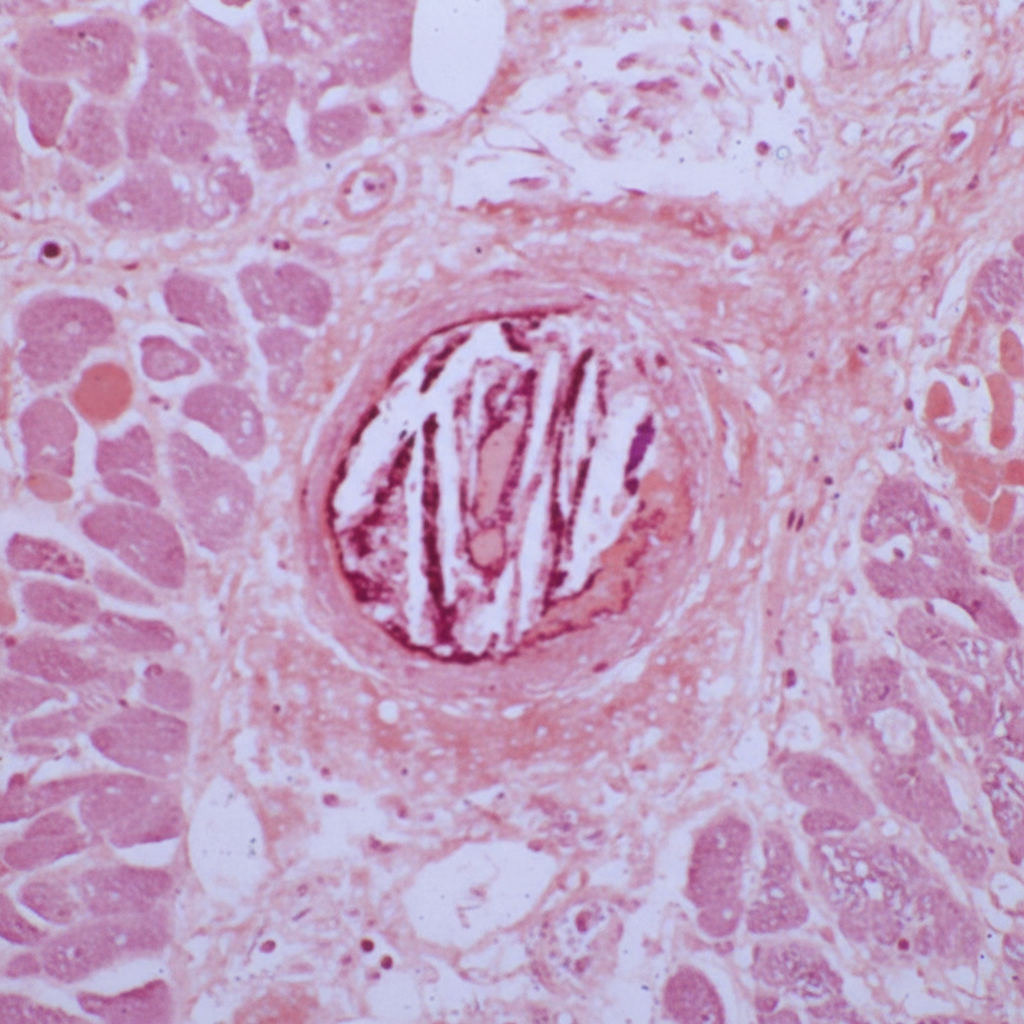
Two weeks after undergoing an emergency cardiac catheterization for unstable angina pectoris, a 65-year-old man has decreased urinary output. He takes naproxen for osteoarthritis and was started on aspirin, clopidogrel, and metoprolol after the coronary intervention. His temperature is 38.1°C (100.5°F), pulse is 96/min, and blood pressure is 128/88 mm Hg. Examination shows mottled, reticulated purplish discoloration of the feet and ischemic changes on the right big toe. His leukocyte count is 16,500/mm3 with 56% segmented neutrophils, 12% eosinophils, 30% lymphocytes, and 2% monocytes. His serum creatinine concentration is 4.5 mg/dL. A photomicrograph of a kidney biopsy specimen is shown. Which of the following is the most likely cause of this patient's presentation?
A 25-year-old previously healthy woman is admitted to the hospital with progressively worsening shortness of breath. She reports a mild fever. Her vital signs at the admission are as follows: blood pressure 100/70 mm Hg, heart rate 111/min, respiratory rate 20/min, and temperature 38.1℃ (100.6℉); blood saturation on room air is 90%. Examination reveals a bilateral decrease of vesicular breath sounds and rales in the lower lobes. Plain chest radiograph demonstrates bilateral opacification of the lower lobes. Despite appropriate treatment, her respiratory status worsens. The patient is transferred to the intensive care unit and put on mechanical ventilation. Adjustment of which of the following ventilator settings will only affect the patient’s oxygenation?
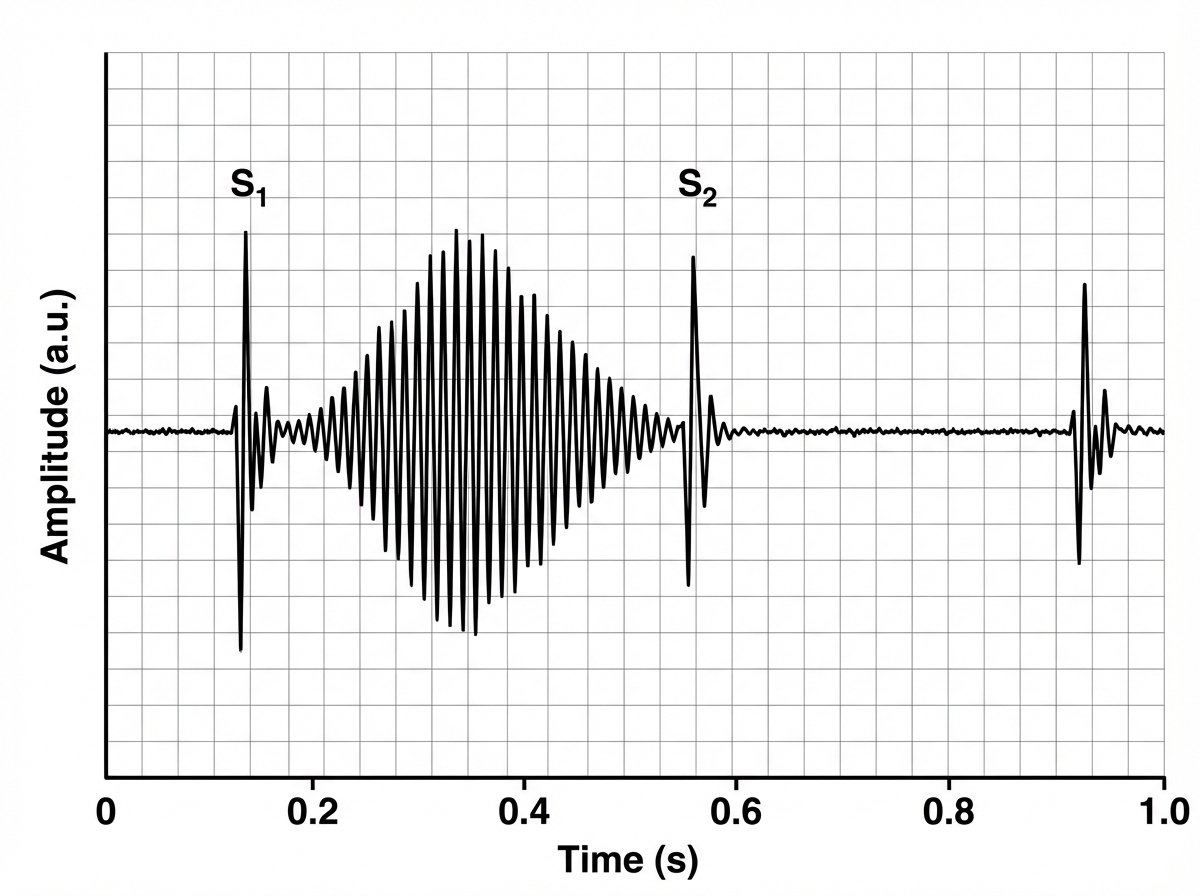
A healthy 20-year-old African American man presents to the clinic for pre-participation sports physical for college football. He has no health complaints at this time. He has no recent history of illness or injury. He denies chest pain and palpitations. He reports no prior syncopal episodes. He had surgery 2 years ago for appendicitis. His mother is healthy and has an insignificant family history. His father had a myocardial infarction at the age of 53, and his paternal uncle died suddenly at the age of 35 for unknown reasons. His temperature is 37.1°C (98.8°F), the heart rate is 78/min, the blood pressure is 110/66 mm Hg, and the respiratory rate is 16/min. He has a tall, proportional body. There are no chest wall abnormalities. Lungs are clear to auscultation. His pulse is 2+ and regular in bilateral upper and lower extremities. His PMI is nondisplaced. Auscultation of his heart in the 5th intercostal space at the left midclavicular line reveals the following sound; the murmur is noted to increase in intensity with Valsalva maneuver and upon standing. Which of the following is the most concerning potential complication of this patient's cardiac findings?
A 76-year-old woman with hypertension and coronary artery disease is brought to the emergency department after the sudden onset of right-sided weakness. Her pulse is 83/min and blood pressure is 156/90 mm Hg. Neurological examination shows right-sided facial drooping and complete paralysis of the right upper and lower extremities. Tongue position is normal and she is able to swallow liquids without difficulty. Knee and ankle deep tendon reflexes are exaggerated on the right. Sensation to vibration, position, and light touch is normal bilaterally. She is oriented to person, place, and time, and is able to speak normally. Occlusion of which of the following vessels is the most likely cause of this patient's current symptoms?
A 57-year-old woman presents to her primary care physician with a concern for joint pain. She states that she often feels minor joint pain and morning stiffness in both of her hands every day, particularly in the joints of her fingers. Her symptoms tend to improve as the day goes on and she states they are not impacting the quality of her life. She lives alone as her partner recently died. She smokes 1 pack of cigarettes per day and drinks 2-3 alcoholic drinks per day. Her last menses was at age 45 and she works at a library. The patient has a history of diabetes and chronic kidney disease with her last GFR at 45 mL/min. Her temperature is 97.5°F (36.4°C), blood pressure is 117/58 mmHg, pulse is 90/min, respirations are 14/min, and oxygen saturation is 98% on room air. Physical examination is within normal limits. Which of the following interventions is appropriate management of future complications in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app