
Cardiology — MCQs

On this page
A 58-year-old man is diagnosed with right lower lobe pneumonia and has been admitted to a tertiary care hospital. His laboratory investigations suggest that he acquired an infection from the hospital where he underwent an elective abdominal surgery 3 weeks ago. His past medical records reveal a history of deep vein thrombosis and pulmonary embolism one year prior. After a steady clinical improvement over 5 days of inpatient treatment, he develops a cough, breathlessness, and hemoptysis on the 6th day. His temperature is 38.6°C (101.5°F), the pulse is 112/min, the blood pressure is 130/84 mm Hg, and the respiratory rate is 28/min. A general examination shows the presence of edema over the right leg and tenderness over the right calf region. Auscultation of the chest reveals localized crackles over the left mammary region and right infrascapular region. However, his heart sounds are normal, except for the presence of tachycardia, and there are no murmurs. Which of the following is the investigation of choice as the immediate next step in this patient’s management?
A 52-year-old man is admitted directly from the clinic for a serum glucose of 980 mg/dL. He has had type 2 diabetes for 16 years, for which he was prescribed metformin and glimepiride; however, he reports not having followed his prescription due to its high cost. For the past 12 days, he has had excess urination, and has lost 6 kg in weight. He has also noted a progressively worsening cough productive of greenish-brown sputum for approximately 20 days. His temperature is 38.9°C (102.02°F), blood pressure is 97/62 mm Hg, pulse is 97/minute and respiratory rate is 26/minute. On physical examination, he is somnolent, his eyes are sunken, and there are crackles at the left lung base. Lab results are shown: Arterial pH: 7.33 Serum sodium: 130 mEq/L Serum potassium: 3 mEq/L Serum osmolality: 325 mOsm/kg Serum beta-hydroxybutyrate: negative Urinalysis: trace ketones Intravenous normal saline infusion is started. Which of the following is the best next step in this patient?
A 75-year-old woman comes to the physician because of a 6-month history of fatigue. During this period, she has had fever, pain in both shoulders and her hips, and a 5-kg (11-lb) weight loss. She also reports feeling stiff for about an hour after waking up. She has a history of hypertension and hypercholesterolemia. There is no family history of serious illness. She has smoked a pack of cigarettes daily for the past 50 years. Her medications include hydrochlorothiazide and atorvastatin. She appears pale. Her temperature is 38°C (100.4°F), pulse is 90/min, and blood pressure is 135/85 mm Hg. Range of motion of the shoulders and hips is reduced due to pain. Examination shows full muscle strength. The remainder of the examination shows no abnormalities. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h and a C-reactive protein concentration of 25 mg/dL (N=0–10 mg/dL). Which of the following is the most appropriate next step in management?
An otherwise healthy 57-year-old man presents to the emergency department because of progressive shortness of breath and exercise intolerance for the past 5 days. He denies recent travel or illicit habits. His temperature is 36.7°C (98.1°F), the blood pressure is 88/57 mm Hg, and the pulse is 102/min. The radial pulse weakens with inspiration. Physical examination reveals bilateral 1+ pedal edema. There is jugular venous distention at 13 cm and muffled heart sounds. Transthoracic echocardiogram shows reciprocal respiratory ventricular inflow and ventricular diastolic collapse. Which of the following is the best next step in the management of this patient condition?
A 70-year-old man presents to a physician with a cough and difficulty breathing during the last 7 years. He has smoked since his teenage years and regularly inhales tiotropium, formoterol, and budesonide and takes oral theophylline. The number of exacerbations has been increasing over the last 6 months. His temperature is 37.2°C (99°F), the heart rate is 92/min, the blood pressure is 134/88 mm Hg and the respiratory rate is 26/min. On chest auscultation breath sounds are diffusely decreased and bilateral rhonchi are present. Pulse oximetry shows his resting oxygen saturation to be 88%. Chest radiogram shows a flattened diaphragm, hyperlucency of the lungs, and a long, narrow heart shadow. The physician explains this condition to the patient and emphasizes the importance of smoking cessation. In addition to this, which of the following is most likely to reduce the risk of mortality from the condition?
A 62-year-old man comes to the physician because of a 1-day history of dull pain and stiffness of the right knee. He takes chlorthalidone for hypertension. Physical examination of the right knee shows a large effusion and mild erythema; range of motion is limited by pain. Arthrocentesis of right knee yields a cloudy aspirate. Gram stain is negative. Analysis of the synovial fluid shows a leukocyte count of 15,000/mm3 and 55% neutrophils. Microscopic examination of the synovial fluid under polarized light shows positively birefringent rhomboid crystals. Further evaluation of this patient is most likely to show which of the following findings?
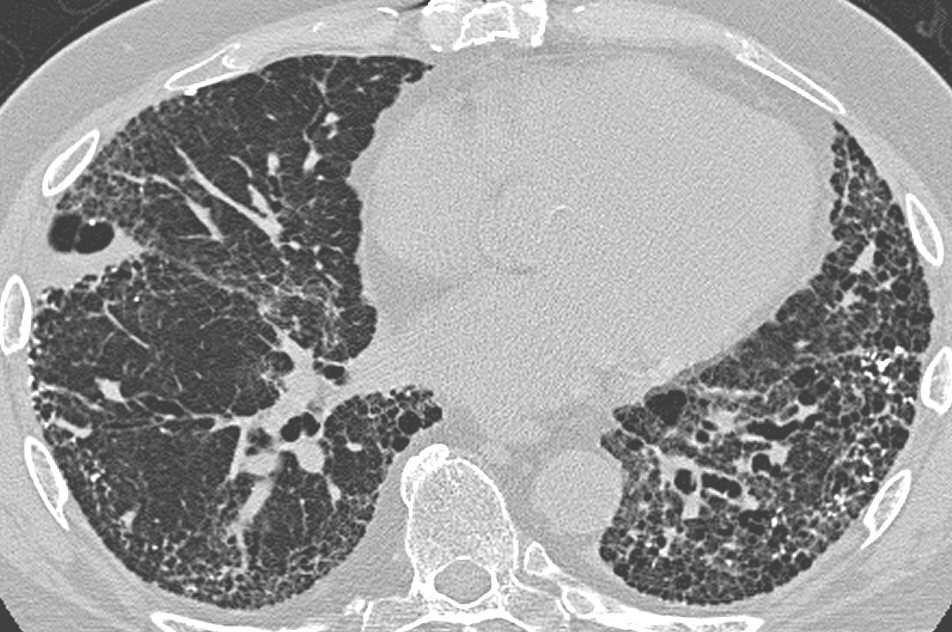
A 75-year-old man is evaluated in the emergency department for increasing shortness of breath for the last 8 months. He also complains of a dry cough for the last 6 months. Initially, his shortness of breath occurs with exertion, but now he feels it at rest as well. He has no other complaints. He has a sedentary lifestyle and had a hip replacement surgery recently. The past medical history is significant for hypertension for which he is taking lisinopril. The patient is a lifetime non-smoker. The blood pressure is 135/85 mm Hg, pulse rate is 85/min, and the temperature is 36.6°C (97.9°F). Physical examination reveals fine inspiratory crackles and digital clubbing. A chest X-ray reveals peripheral reticular opacities associated with traction bronchiectasis predominantly at the lung bases. The pulmonary function test results reveal a decreased FEV1, a decreased FVC, and a preserved FEV1/FVC ratio. High-resolution CT scan of the chest is shown. Which of the following is the most likely diagnosis?
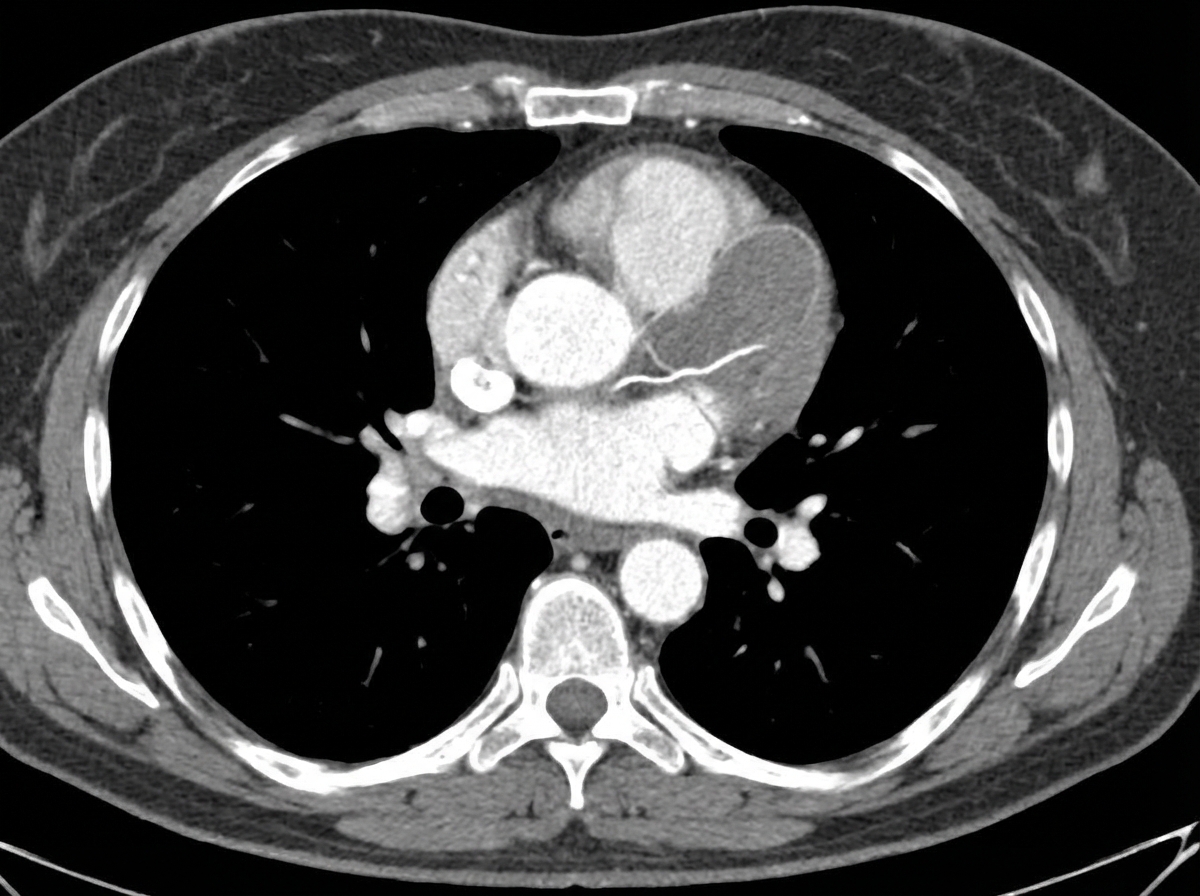
A 58-year-old man is brought to the emergency department by his wife 30 minutes after the sudden onset of severe retrosternal chest pain radiating to his back. He has a history of hyperlipidemia, hypertension, and type 2 diabetes mellitus. He has smoked one-half pack of cigarettes daily for 20 years. Medications include aspirin, captopril, atorvastatin, and metformin. His pulse is 80/min and blood pressure is 160/60 mm Hg. A CT scan of the chest is shown. Which of the following is the strongest predisposing factor for this patient's current condition?
A 37-year old man is being evaluated due to a recent history of fatigue that started 3 weeks ago. The patient presents with a history of HIV, which was first diagnosed 7 years ago. He has been on an antiretroviral regimen and takes it regularly. His CD4+ count is 350 cells/mm3. According to the patient, his partner passed away from a "blood cancer", and he is worried that his fatigue might be connected to a similar pathology. The physician clarifies that there is an increased risk for HIV patients to develop certain kinds of lymphomas. Which one of the conditions below is the patient more likely to develop based on his medical history?
A 67-year-old man presents to the emergency department with acute onset of shortness of breath of 30 minutes' duration. Initially, he felt faint but did not lose consciousness. He is complaining of left-sided chest pain that increases on deep inspiration. He has no history of cardiopulmonary disease. A week ago, he underwent a total left hip replacement and, following discharge, was on bed rest for 5 days due to poorly controlled pain. He subsequently noticed swelling in his right calf, which is tender on examination. His current vital signs reveal a temperature of 38.0°C (100.4°F), heart rate of 112/min, blood pressure of 95/65 mm Hg, and an oxygen saturation on room air of 91%. Computerized tomography pulmonary angiography (CTPA) shows a partial intraluminal filling defect. Which of the following is the mechanism of this patient's illness?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app