
Cardiology — MCQs

On this page
A 54-year-old man is brought to the emergency department after having been hit by a car while riding his bicycle. He was not wearing a helmet. Despite appropriate life-saving measures, he dies 2 hours later because of a severe intracranial hemorrhage. Autopsy of the heart shows general thickening of the left ventricular wall with narrowing of the ventricular chamber. Which of the following conditions is the most likely underlying cause of the described cardiac changes?
A 39-year-old female with poorly controlled systemic lupus erythematosus (SLE) presents to the emergency room with a cough and pleuritic chest pain. She states that she developed these symptoms 2 days prior. The pain appears to improve when the patient leans forward. She currently takes hydroxychloroquine for her systemic lupus erythematosus but has missed several doses recently. Her temperature is 99°F (37.2°C), blood pressure is 135/80 mmHg, pulse is 115/min, and respirations are 22/min. Physical examination reveals a rise in jugular venous pressure during inspiration. In addition to tachycardia, which of the following EKG patterns is most likely to be seen in this patient?
A 55-year-old man presents to the internal medicine clinic with complaints of numbness and tingling in his fingers that he first noticed 6 months ago. It has been progressively worsening and has reached the point where it is affecting his normal daily activities, such as brushing his teeth. His past medical history is significant for sinusitis and allergic rhinitis since the age of 18, as well as episodic wheezing and shortness of breath since he was 30. He was diagnosed with asthma when he was 22 years old, and subsequently with gastroesophageal reflux disease (GERD) when he was 40. His current medications include albuterol, loratadine, mometasone, and omeprazole. His blood pressure is 128/86 mm Hg, heart rate is 78/min, and respiratory rate is 16/min. On physical exam, the patient’s skin is mottled and appears to have a diffuse, lace-like, erythematous discoloration of the arms, legs, and trunk. There is also a small papular rash on his right forearm. Bilateral wheezes are heard on auscultation. Which of the following is the most likely diagnosis?
A 42-year-old man presents to his dermatologist with a rash on the extensor surfaces of his elbows and knees which has occurred episodically ever since he was a teenager. The patient was recently diagnosed with essential hypertension and was prescribed lisinopril by his primary care physician. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 128/91 mm Hg, and heart rate 82/min. The physical examination reveals sharply demarcated, erythematous plaques with silvery-white scales on the back of his elbows and front of his knees. He has less than 3% of the total body surface area affected. Which of the following is the best initial therapy for this patient’s condition?
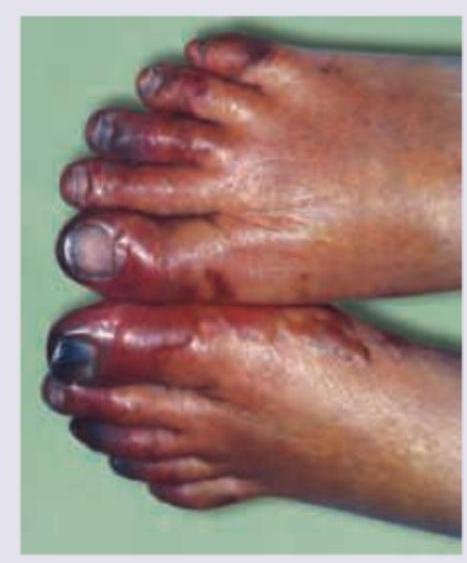
A 72-year-old man comes to the emergency department because of severe, acute, right leg pain for 2 hours. The patient's symptoms started suddenly while he was doing household chores. He has no history of leg pain at rest or with exertion. Yesterday, he returned home after a 6-hour bus ride from his grandson's home. He has hypertension treated with ramipril. He appears uncomfortable. His temperature is 37.4°C (99.3°F), pulse is 105/min and irregular, and blood pressure is 146/92 mm Hg. The right lower extremity is cool and tender to touch. A photograph of the limb is shown. Femoral pulses are palpable bilaterally; popliteal and pedal pulses are decreased on the right side. Sensation to pinprick and light touch and muscle strength are decreased in the right lower extremity. Which of the following is most likely to confirm the underlying source of this patient's condition?
A 55-year-old man presents to his primary care physician for a wellness checkup. He states that he generally feels well and has no complaints at this time. The patient consumes alcohol frequently, eats a high sodium diet, and is sedentary. His temperature is 97.5°F (36.4°C), blood pressure is 167/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. The patient is 5'10" tall and weighs 220 lbs (BMI 31.5 kg/m²). The patient's blood pressure at his last 2 appointments were 159/100 mmHg and 162/99 mmHg, respectively. His physician wants to intervene to manage his blood pressure. Which of the following is the most effective lifestyle intervention for this patient's hypertension?
A 38-year-old woman is referred to a cardiologist for evaluation of syncope. Over the past year she has experienced 2 syncopal events. The first event occurred while she was standing, and the second when she laid down on her side. She denies bowel or bladder incontinence during the episodes or palpitations. However, she reports the presence of a low-grade fever over the past 3 months and a recent visit to the emergency department for a transient ischemic attack. She has a history of intravenous drug use but reports not having used in over 5 years. Temperature is 100.0°F (37.8°C), blood pressure is 115/72 mmHg, pulse is 90/min, and respirations are 20/min and regular. A detailed neurologic examination reveals no focal deficits. Cardiac auscultation demonstrates a diastolic "plop" at the cardiac apex. Which of the following findings will most likely be demonstrated on transthoracic echocardiography?
A 27-year-old woman presents to her primary care physician because of headaches that she has had over the last three weeks. She has not had any significant past medical history though she does recall that various types of cancer run in her family. She has also noticed that she has been gaining some weight, and her feet no longer fit into her favorite shoes. On presentation, her temperature is 98.6°F (37°C), blood pressure is 159/92 mmHg, pulse is 75/min, and respirations are 16/min. Physical exam reveals 1+ edema in her lower extremities bilaterally. She is placed on captopril and presents to the emergency department two weeks later after a minor motor vehicle accident. She is cleared of any serious injuries, and as part of her workup, labs are drawn with the following results: BUN: 47 mg/dL Creatinine: 1.4 mg/dL Which of the following findings would most likely also be seen in this patient?
A 33-year-old man presents with his recent laboratory results. He has no symptoms currently, but he underwent a medical evaluation as a requirement for taking up a new job. His medical history is not significant. His laboratory reports are as follows: Blood hemoglobin 13.7 g/dL Leukocyte count 8,000/mm3 Platelet count 350,000/mm3 Serum creatinine 0.8 mg/dL Serum alanine aminotransferase 16 U/L Serum aspartate aminotransferase 14 U/L Serum cholesterol 450 mg/dL Serum triglyceride 790 mg/dL Serum LDL cholesterol 150 mg/dL Serum HDL cholesterol 55 mg/dL Which of the following findings is most likely to be present on physical examination of this patient?
A 58-year-old patient comes to the physician because of progressive pain and swelling of his left calf for the past 2 days. He has no personal or family history of serious illness. He does not smoke or drink alcohol. His last digital rectal examination and colonoscopy at the age of 50 years were normal. His vital signs are within normal limits. He is 183 cm (6 ft) tall and weighs 80 kg (176 lb); BMI is 24 kg/m2. Physical examination shows redness, warmth, and tenderness of the left calf. The circumference of the left lower leg is 4 cm greater than the right. Dorsiflexion of the left foot elicits pain in the ipsilateral calf. Laboratory studies show: Hemoglobin 15 g/dL Leukocyte count 9000/mm3 Platelet count 190,000/mm3 Erythrocyte sedimentation rate 12 mm/h Serum Urea nitrogen 18 mg/dL Creatinine 1.0 mg/dL Alkaline phosphatase 24 U/L Aspartate aminotransferase (AST, GOT) 12 U/L Alanine aminotransferase (ALT, GPT) 10 U/L Urine Protein negative RBC 1/hpf WBC none Compression ultrasonography with Doppler shows a non-compressible left popliteal vein with a visible 0.5-cm hyperechoic mass and reduced flow. In addition to initiating anticoagulation, which of the following is the most appropriate next step in management?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app