
Cardiology — MCQs

On this page
A 36-year-old woman comes to the gynecologist because of a 4-month history of irregular menstrual cycles. Menses occur at irregular 15 to 45-day intervals and last 1–2 days with minimal flow. She also reports a milk-like discharge from her nipples for 3 months, as well as a history of fatigue and muscle and joint pain. She does not have abdominal pain, fever, or headache. She has recently gained 2.5 kg (5.5 lb) of weight. She was diagnosed with schizophrenia and started on aripiprazole by a psychiatrist 8 months ago. She has hypothyroidism but has not been taking levothyroxine for 6 months. She does not smoke or consume alcohol. She appears healthy and anxious. Her vital signs are within normal limits. Pelvic examination shows vaginal atrophy. Visual field and skin examination are normal. Laboratory studies show: Hemoglobin 12.7 g/dL Serum Glucose 88 mg/dL Creatinine 0.7 mg/dL Thyroid-stimulating hormone 16.3 μU/mL Cortisol (8AM) 18 μg/dL Prolactin 88 ng/mL Urinalysis is normal. An x-ray of the chest and ultrasound of the pelvis show no abnormalities. Which of the following is the most likely explanation for the nipple discharge in this patient?
A 69-year-old male presents to his primary care provider for a general checkup. The patient currently has no complaints. He has a past medical history of diabetes mellitus type II, hypertension, depression, obesity, and a myocardial infarction seven years ago. The patient's prescribed medications are metoprolol, aspirin, lisinopril, hydrochlorothiazide, fluoxetine, metformin, and insulin. The patient states that he has not been filling his prescriptions regularly and that he can not remember what medications he has been taking. His temperature is 99.5°F (37.5°C), pulse is 96/min, blood pressure is 180/120 mmHg, respirations are 18/min, and oxygen saturation is 97% on room air. Serum: Na+: 139 mEq/L K+: 4.3 mEq/L Cl-: 100 mEq/L HCO3-: 24 mEq/L BUN: 7 mg/dL Glucose: 170 mg/dL Creatinine: 1.2 mg/dL On physical exam which of the following cardiac findings would be expected?
A 63-year-old woman comes to the physician with a 3-month history of progressively worsening right calf pain. She reports that the pain occurs after walking for about 10 minutes and resolves when she rests. She has hypertension and hyperlipidemia. She takes lisinopril and simvastatin daily. She has smoked two packs of cigarettes daily for 34 years. Her pulse is 78/min and blood pressure is 142/96 mm Hg. Femoral and popliteal pulses are 2+ bilaterally. Left pedal pulses are 1+; right pedal pulses are absent. Remainder of the examination shows no abnormalities. Ankle-brachial index (ABI) is 0.65 in the right leg and 0.9 in the left leg. This patient is at greatest risk of which of the following conditions?
A 53-year-old woman comes to the physician because of pain in her ankle. She twisted her right ankle inward when walking on uneven ground the previous day. She describes the pain as 6 out of 10 in intensity. She is able to bear weight on the ankle and ambulate. Three weeks ago, she had an episode of gastroenteritis that lasted for two days and resolved spontaneously. She has type 2 diabetes mellitus, hypertension, and hyperlipidemia. Her father has type 2 diabetes mellitus and chronic renal failure. Her mother has hypothyroidism and a history of alcohol abuse. The patient drinks 8–10 beers each week and does not smoke or use illicit drugs. She adheres to a strict vegetarian diet. Current medications include metformin, atorvastatin, and lisinopril. Her temperature is 36.9°C (98.4°F), heart rate is 84/min, and blood pressure is 132/80 mm Hg. Examination of the right ankle shows edema along the lateral aspect. She has pain with eversion and tenderness to palpation on the lateral malleolus. The foot is warm to touch and has dry skin. Pedal pulses are palpable. She has decreased sensation to light touch on the plantar and dorsal aspects of the big toe. She has full range of motion with 5/5 strength in flexion and extension of the big toe. Laboratory studies show: Hemoglobin 15.1 g/dL Hemoglobin A1c 8.1% Leukocyte count 7,200/mm3 Mean corpuscular volume 82 μm3 Serum Na+ 135 mEq/L K+ 4.0 mEq/L Cl- 101 mEq/L Urea nitrogen 24 mg/dL Creatinine 1.3 mg/dL Thyroid-stimulating hormone 1.2 μU/mL Which of the following is the most likely cause of the decreased sensation in this patient?
A 29-year-old woman presents with a skin rash that has spread on her arm over the last few days. She also complains of fever, headache, joint pain, and stiffness of the neck associated with the onset of the rash. On physical examination, there is an annular, red rash with a clear area in the center similar to a bull's-eye (see image). The patient says she went on a camping trip to Connecticut last month but does not remember being bitten by an insect. Which of the following neurologic complications could result if this condition remains untreated in this patient?

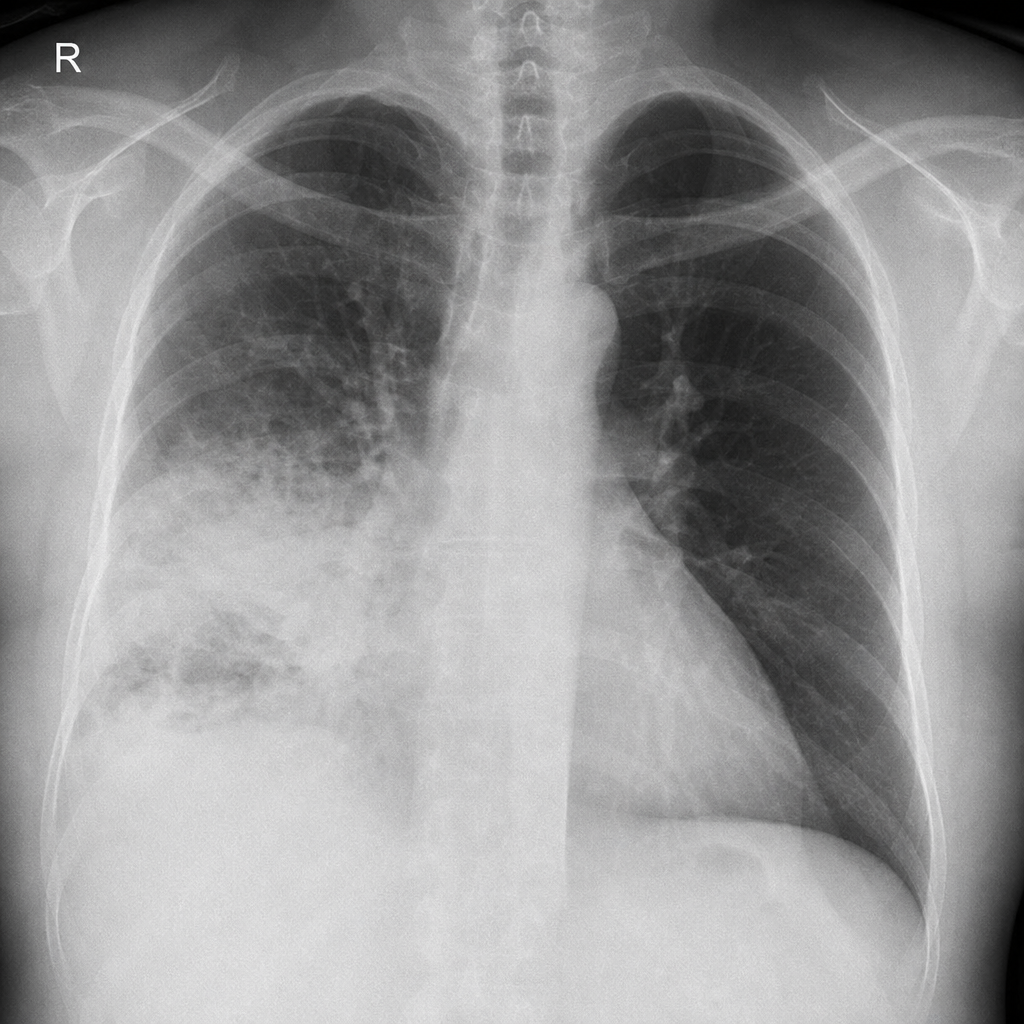
A 67-year-old woman is brought to the emergency department for the evaluation of fever, chest pain, and a cough productive of a moderate amount of greenish-yellow sputum for 2 days. During this period, she has had severe malaise, chills, and difficulty breathing. She has hypertension, hypercholesterolemia, and type 2 diabetes mellitus. She smoked one pack of cigarettes daily for 20 years, but quit 5 years ago. Current medications include simvastatin, captopril, and metformin. Temperature is 39°C (102.2°F), pulse is 110/min, respirations are 33/min, and blood pressure is 143/88 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 94%. Crackles are heard on auscultation of the right middle/lower lung. Laboratory studies show a leukocyte count of 12,300/mm3, an erythrocyte sedimentation rate of 60 mm/h, and a urea nitrogen of 15 mg/dL. A chest x-ray is shown. Which of the following is the most appropriate next step in the management of this patient?
A 37-year-old woman comes to the physician because of irregular menses and generalized fatigue for the past 4 months. Menses previously occurred at regular 25- to 29-day intervals and lasted for 5 days but now occur at 45- to 60-day intervals. She has no history of serious illness and takes no medications. She is 155 cm (5 ft 1 in) tall and weighs 89 kg (196 lb); BMI is 37 kg/m2. Her temperature is 37°C (98.6°F), pulse is 90/min, and blood pressure is 146/100 mm Hg. Examination shows facial hair as well as comedones on the face and back. There are multiple ecchymotic patches on the trunk. Neurological examination shows weakness of the iliopsoas and biceps muscles bilaterally. Laboratory studies show: Hemoglobin 13.1 g/dL Leukocyte count 13,500/mm3 Platelet count 510,000/mm3 Serum Na+ 145 mEq/L K+ 3.3 mEq/L Cl- 100 mEq/L Glucose 188 mg/dL Which of the following is the most likely diagnosis?
A 27-year-old man presents to the emergency department for altered mental status. The patient was found napping in a local market and brought to the hospital. The patient has a past medical history of polysubstance abuse and is homeless. His temperature is 104°F (40.0°C), blood pressure is 100/52 mmHg, pulse is 133/min, respirations are 25/min, and oxygen saturation is 99% on room air. Physical exam is notable for an altered man. Cardiopulmonary exam reveals a murmur over the left lower sternal border. A bedside ultrasound reveals a vegetation on the tricuspid valve. The patient is ultimately started on IV fluids, norepinephrine, vasopressin, vancomycin, and piperacillin-tazobactam. A central line is immediately placed in the internal jugular vein and the femoral vein secondary to poor IV access. Cardiothoracic surgery subsequently intervenes to remove the vegetation. While recovering in the ICU, days 3-5 are notable for an improvement in the patient’s symptoms. Two additional peripheral IVs are placed while in the ICU on day 5, and the femoral line is removed. On day 6, the patient's fever and hemodynamic status worsen. Though he is currently responding and not complaining of any symptoms including headache, photophobia, neck stiffness, or pain, he states he is feeling weak. Jolt accentuation of headache is negative and his abdominal exam is benign. A chest radiograph, urinalysis, and echocardiogram are unremarkable though the patient’s blood cultures are positive when drawn. Which of the following is the best next step in management?
A 42-year-old man presents to the clinic for a several-month history of fatigue, and it is starting to affect his work. He often needs to sneak away in the middle of the day to take naps or else he cannot focus and is at risk of falling asleep at his desk. He has been feeling like this for approximately 1 year. Otherwise, he feels healthy and takes no medications. On further questioning, he also had constipation and thinks he has gained some weight. He denies shortness of breath, chest pain, lightheadedness, or blood in his stool. The vital signs include: pulse 56/min, blood pressure 124/78 mm Hg, and oxygen saturation 99% on room air. The physical exam is notable only for slightly dry skin. The complete blood count (CBC) is within normal limits, and the thyroid-stimulating hormone (TSH) is 8.0 μU/mL. Which of the following is the next best treatment for this patient?
A 22-year-old woman is brought to the physician by her husband because of a gradual 20-kg (45-lb) weight loss and recurrent episodes of vomiting without diarrhea over the past 2 years. Her last menstrual period was 6 months ago. On physical examination, she appears fatigued and emaciated, and there is bilateral swelling of the retromandibular fossa. Laboratory studies show hypokalemia and a hemoglobin concentration of 8 g/dL. Which of the following additional findings is most likely in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app