
Cardiology — MCQs

On this page
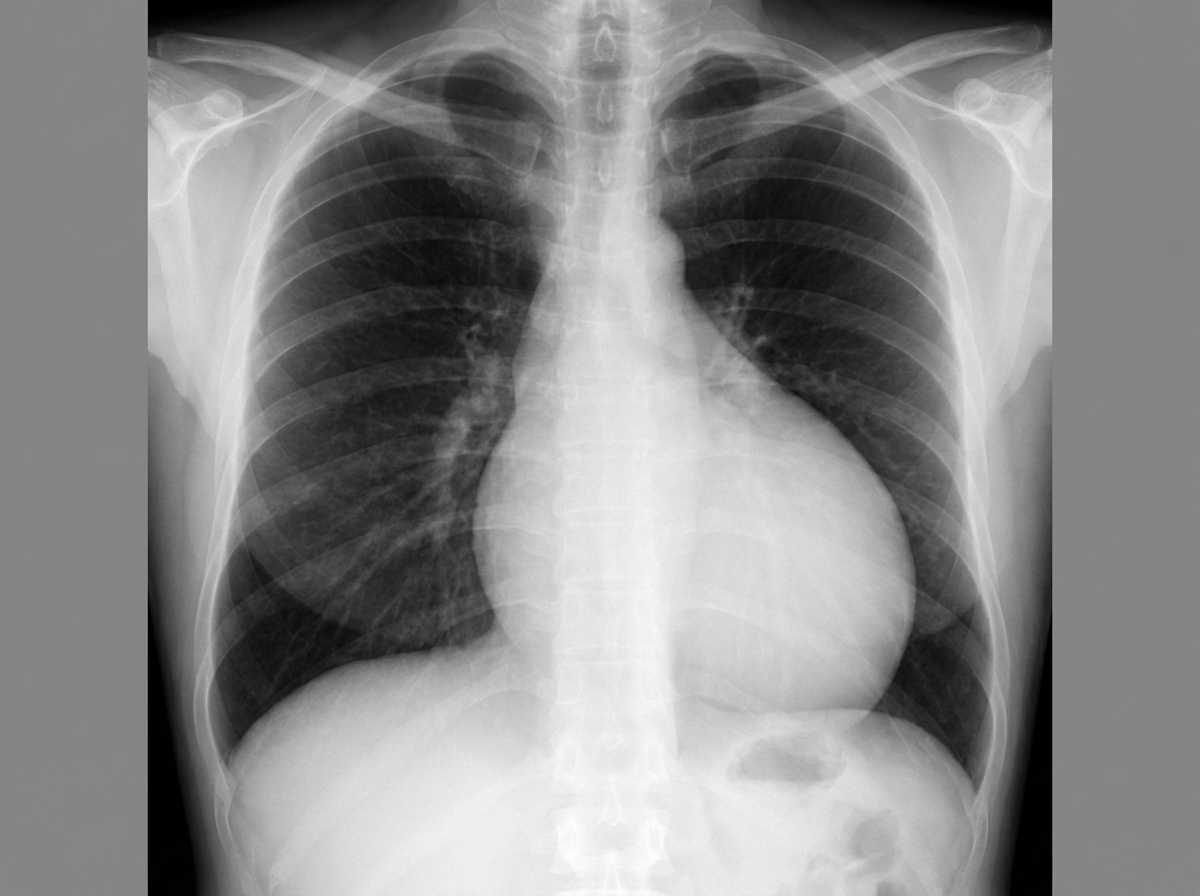
A 49-year-old man comes to the physician because of a 2-week history of increasing shortness of breath. He has also had chest pain that is exacerbated by deep inspiration. He has had recurrent episodes of pain in his fingers for the past 2 years. Two years ago, he was treated for a deep vein thrombosis. He has hypertension and anxiety. Current medications include enalapril, St John's wort, and ibuprofen. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 17/min, and blood pressure is 110/70 mm Hg. Examination shows pale conjunctiva. There is tenderness to palpation of the proximal interphalangeal and metacarpophalangeal joints of both hands. Heart sounds are distant. The lungs are clear to auscultation. Laboratory studies show: Hemoglobin 11.9 g/dL Leukocyte count 4200/mm3 Platelet count 330,000/mm3 Serum Na+ 136 mEq/L K+ 4.3 mEq/L Antinuclear antibodies 1: 320 Anti-Sm antibodies positive Anti-CCP antibodies negative An x-ray of the chest is shown. Which of the following is most likely to be seen on this patient's ECG?
An 18-year-old Caucasian female presents to your clinic because of a recent increase in thirst and hunger. Urinalysis demonstrates elevated glucose. The patient's BMI is 20. Which of the following is the most common cause of death in persons suffering from this patient's illness?
A 78-year-old man presents to his primary care physician for persistent back pain. The patient states that he has had back pain for awhile; however, this past weekend he was helping his son move heavy furniture. Since the move, his symptoms have been more severe. The patient states that the pain is constant and occurs throughout the day. On review of systems, the patient endorses a recent 15 pound weight loss and constipation. His temperature is 99.5°F (37.5°C), blood pressure is 137/79 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Cardiovascular exam is notable for a murmur at the right sternal border that radiates to the carotids. Pulmonary exam reveals mild bibasilar crackles. Musculoskeletal exam is notable for mild midline tenderness of the lower thoracic spine and the upper segment of the lumbar spine. No bruising or signs of external trauma are observable on the back. Symptoms are not exacerbated when the patient is lying down and his straight leg is lifted. Strength is 5/5 in the lower and upper extremities. The patient's sensation is intact bilaterally in his lower and upper extremities. Laboratory values are ordered and return as seen below. Hemoglobin: 11 g/dL Hematocrit: 34% Leukocyte count: 10,500/mm^3 with normal differential Platelet count: 288,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.6 mg/dL Ca2+: 11.8 mg/dL AST: 12 U/L ALT: 12 U/L Which of the following is the most likely diagnosis?
A 55-year-old man with a history of IV drug abuse presents to the emergency department with an altered mental status. He was found unconscious in the park by police. His temperature is 100.0°F (37.8°C), blood pressure is 87/48 mmHg, pulse is 150/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for multiple scars and abscesses in the antecubital fossa. His laboratory studies are ordered as seen below. Serum: Na+: 139 mEq/L Cl-: 105 mEq/L K+: 4.3 mEq/L HCO3-: 19 mEq/L BUN: 20 mg/dL Glucose: 95 mg/dL Creatinine: 1.5 mg/dL Ca2+: 10.2 mg/dL Which of the following is the most appropriate treatment for this patient’s blood pressure and acid-base status?
An 85-year-old woman otherwise healthy presents with left-sided weakness. Her symptoms started 4 hours ago while she was on the phone with her niece. The patient recalls dropping the phone and not being able to pick it up with her left hand. No significant past medical history. No current medications. Physical examination reveals decreased sensation on the left side, worse in the left face and left upper extremity. There is significant weakness of the left upper extremity and weakness and drooping of the lower half of the left face. Ophthalmic examination reveals conjugate eye deviation to the right. A noncontrast CT of the head is unremarkable. The patient is started on aspirin. A repeat contrast CT of the head a few days later reveals an ischemic stroke involving the lateral convexity of right cerebral hemisphere. Which of the following additional findings would most likely be seen in this patient?
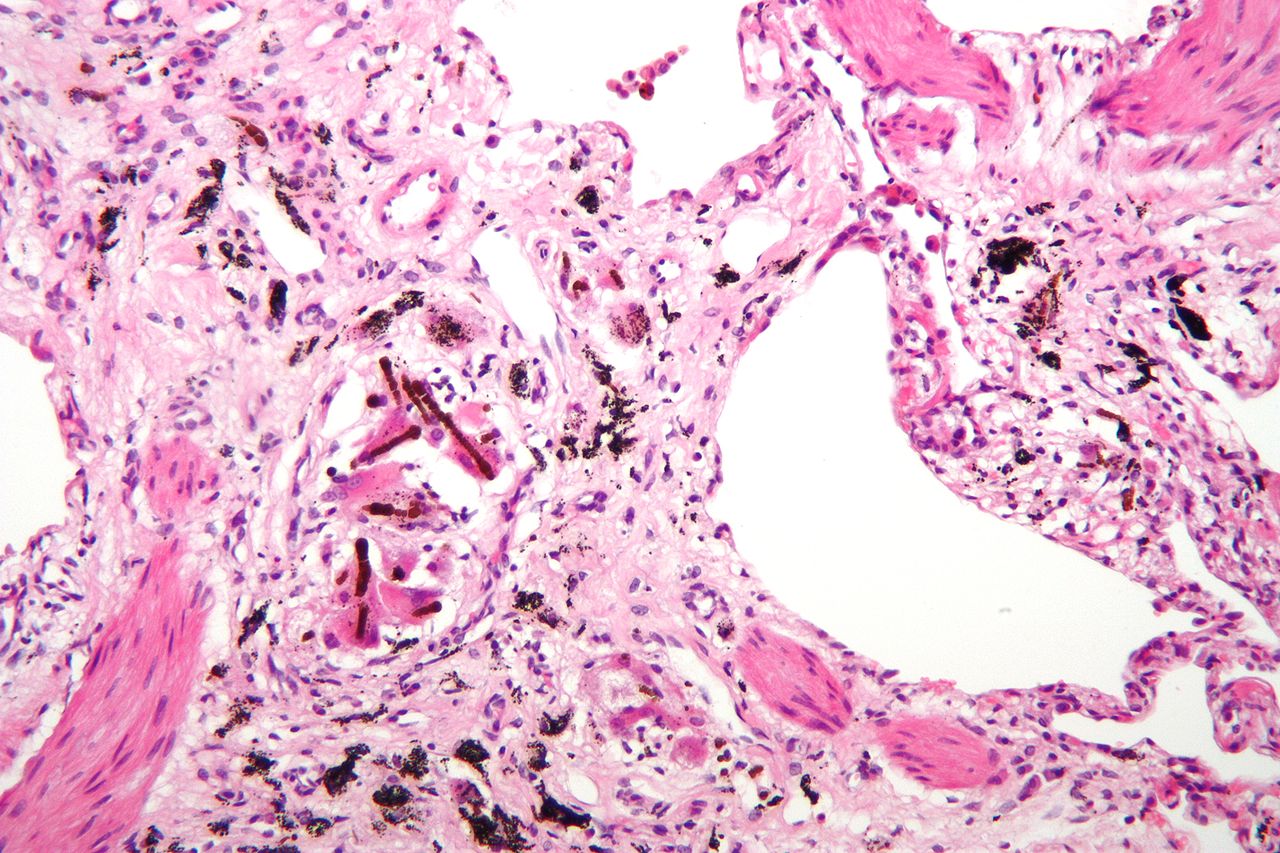
A 61-year-old man comes to the physician because of a 9-month history of progressive shortness of breath on exertion. Pulmonary examinations shows fine bibasilar end-inspiratory crackles. There is digital clubbing. Pulmonary functions tests show an FEV1:FVC ratio of 97% and a total lung capacity of 70%. An x-ray of the chest shows small bilateral reticular opacities, predominantly in the lower lobes. A photomicrograph of a specimen obtained on lung biopsy is shown. The patient most likely works in which of the following fields?
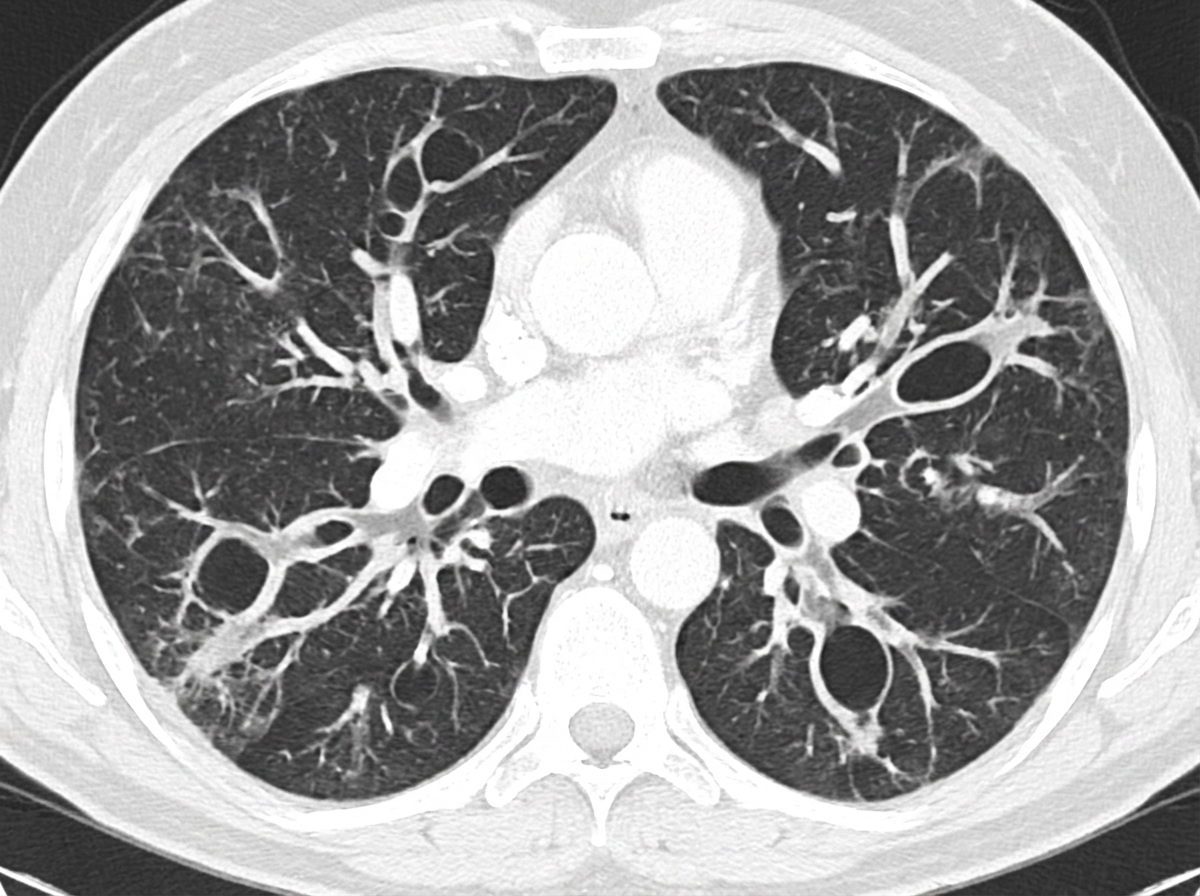
A 47-year-old man comes to the physician because of a 7-week history of cough, shortness of breath, and daily copious sputum production. He has had frequent respiratory tract infections over the past several years. Current medications include dextromethorphan and guaifenesin as needed. He does not smoke cigarettes. His temperature is 37.1°C (98.8°F), pulse is 88/min, respirations are 21/min, and blood pressure is 133/84 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 95%. Diffuse crackles and wheezing are heard on auscultation over bilateral lung fields. A CT scan of the chest is shown. The patient is at greatest risk for which of the following complications?
A 31-year-old woman comes to the physician because of a 2-day history of low-grade intermittent fever, dyspnea, and chest pain that worsens on deep inspiration. Over the past 4 weeks, she has had pain in her wrists and the fingers of both hands. During this period, she has also had difficulties working on her computer due to limited range of motion in her fingers, which tends to be more severe in the morning. Her temperature is 37.7°C (99.8°F). Physical examination shows a high-pitched scratching sound over the left sternal border. Further evaluation of this patient is most likely to reveal which of the following findings?
A 59-year-old man presents to his primary care provider with the complaint of daytime fatigue. He often has a headache that is worse in the morning and feels tired when he awakes. He perpetually feels fatigued even when he sleeps in. The patient lives alone, drinks 2-3 beers daily, drinks coffee regularly, and has a 10 pack-year smoking history. His temperature is 99.0°F (37.2°C), blood pressure is 180/110 mm Hg, pulse is 80/min, respirations are 13/min, and oxygen saturation is 98% on room air. Physical exam is notable for a BMI of 39 kg/m^2. The rest of the patient's pulmonary and neurological exams are unremarkable. Which of the following is the best next step in management?
A 45-year-old woman comes to the physician because of a 3-month history of worsening fatigue, loss of appetite, itching of the skin, and progressive leg swelling. Although she has been drinking 2–3 L of water daily, she has been passing only small amounts of urine. She has type 1 diabetes mellitus, chronic kidney disease, hypertension, and diabetic polyneuropathy. Her current medications include insulin, torasemide, lisinopril, and synthetic erythropoietin. Her temperature is 36.7°C (98°F), pulse is 87/min, and blood pressure is 138/89 mm Hg. She appears pale. There is 2+ pitting edema in the lower extremities. Sensation to pinprick and light touch is decreased over the feet and legs bilaterally. Laboratory studies show: Hemoglobin 11.4 g/dL Leukocyte count 6000/mm3 Platelet count 280,000/mm3 Serum Na+ 137 mEq/L K+ 5.3 mEq/L Cl− 100 mEq/L HCO3− 20 mEq/L Urea nitrogen 85 mg/dL Creatinine 8 mg/dL pH 7.25 Which of the following long-term treatments would best improve quality of life and maximize survival in this patient?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app