
Cardiology — MCQs

On this page
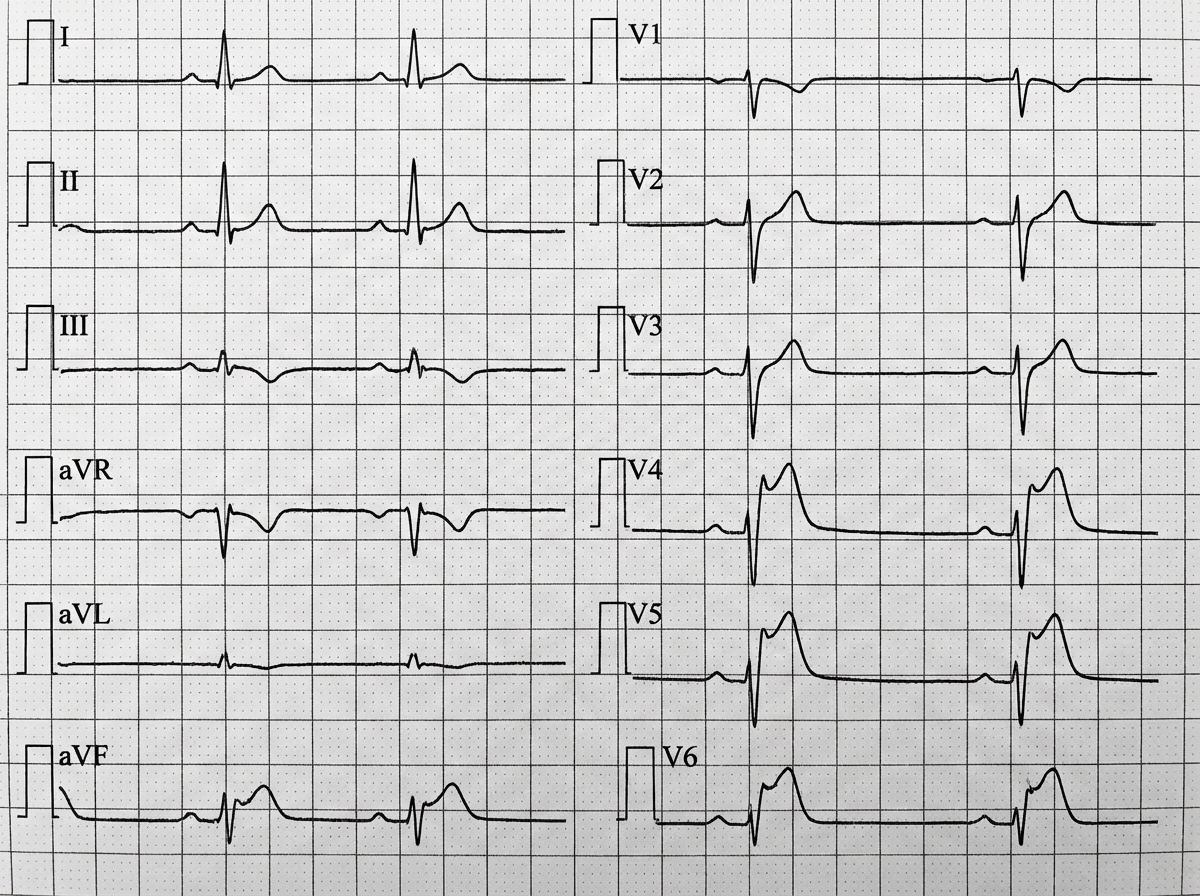
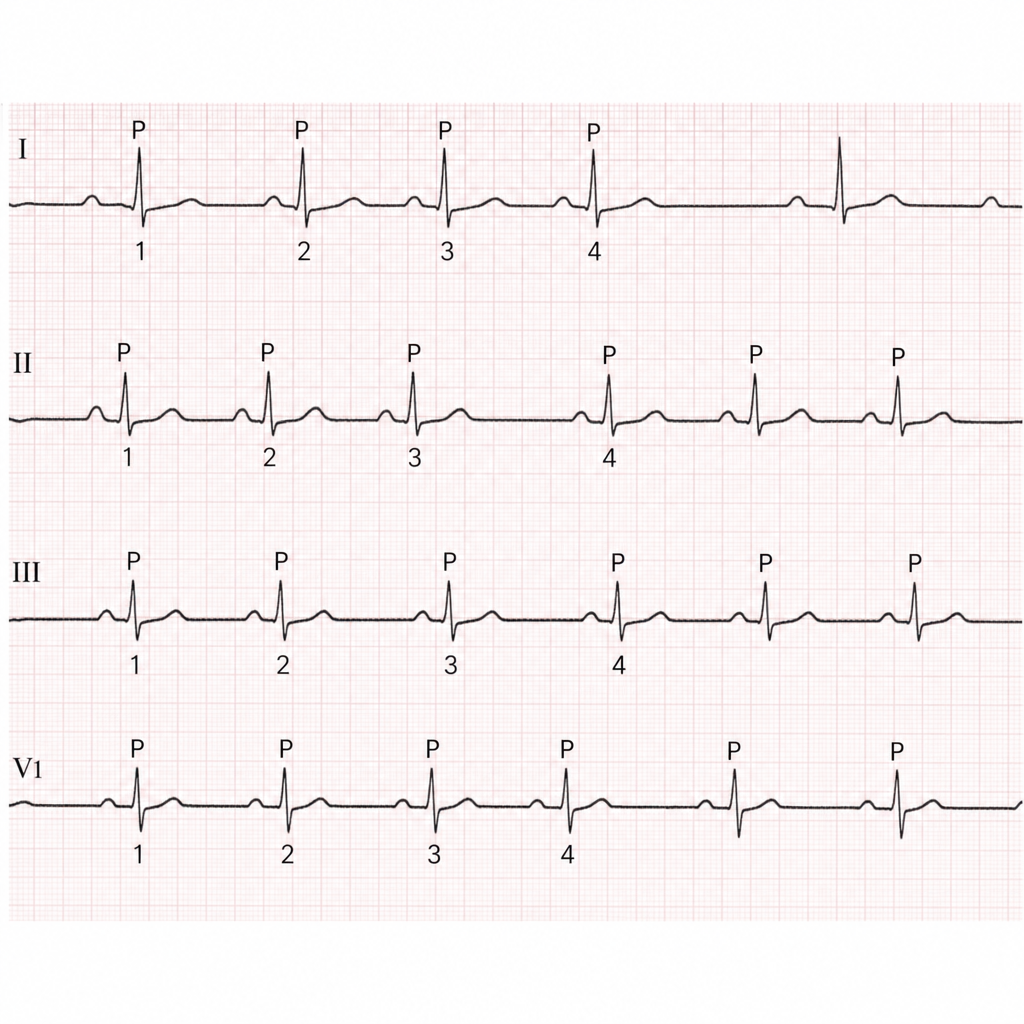
A healthy 36-year-old corporate executive has an ECG performed as part of annual health check-up. He is asymptomatic. ECG shows:
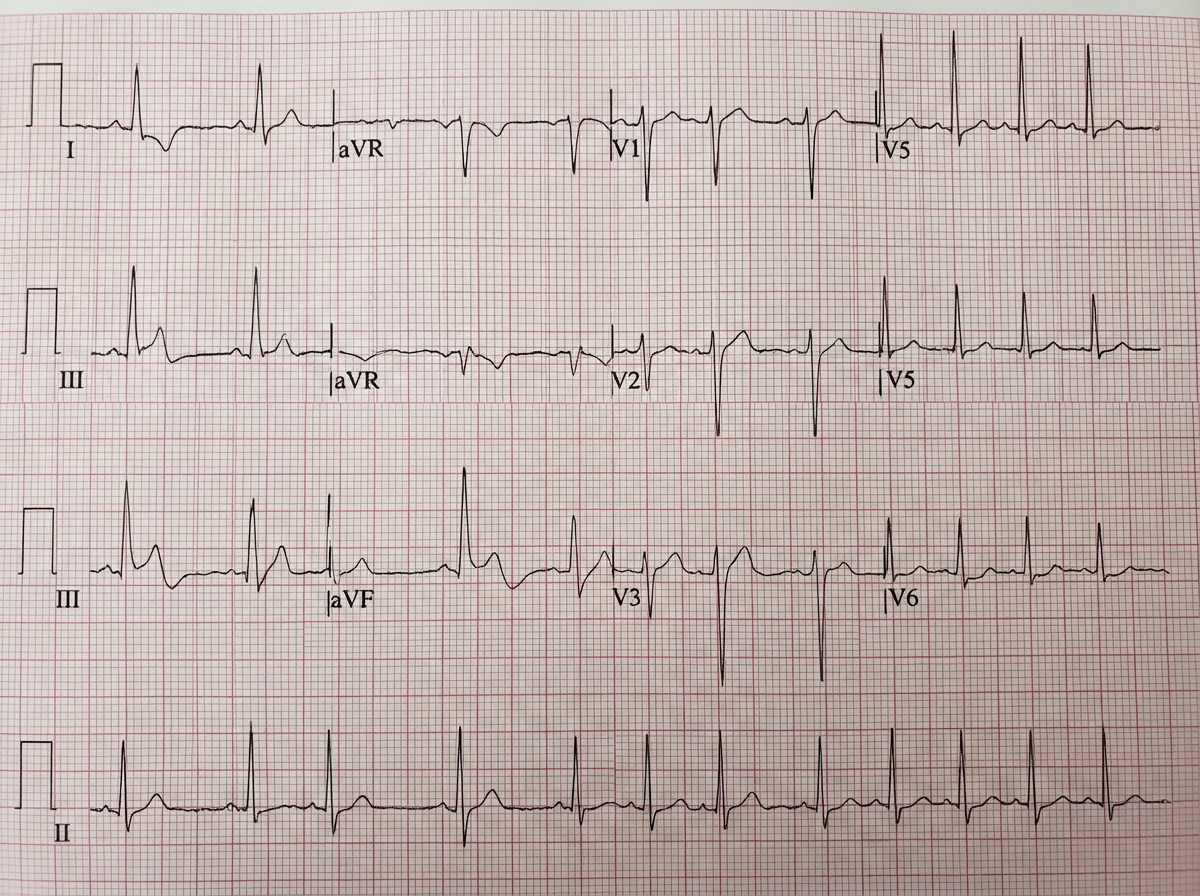
A 50-year-old smoker comes with complaints of ankle edema for last 3 months. The ECG shows all except: (Recent NEET Pattern 2016-17)
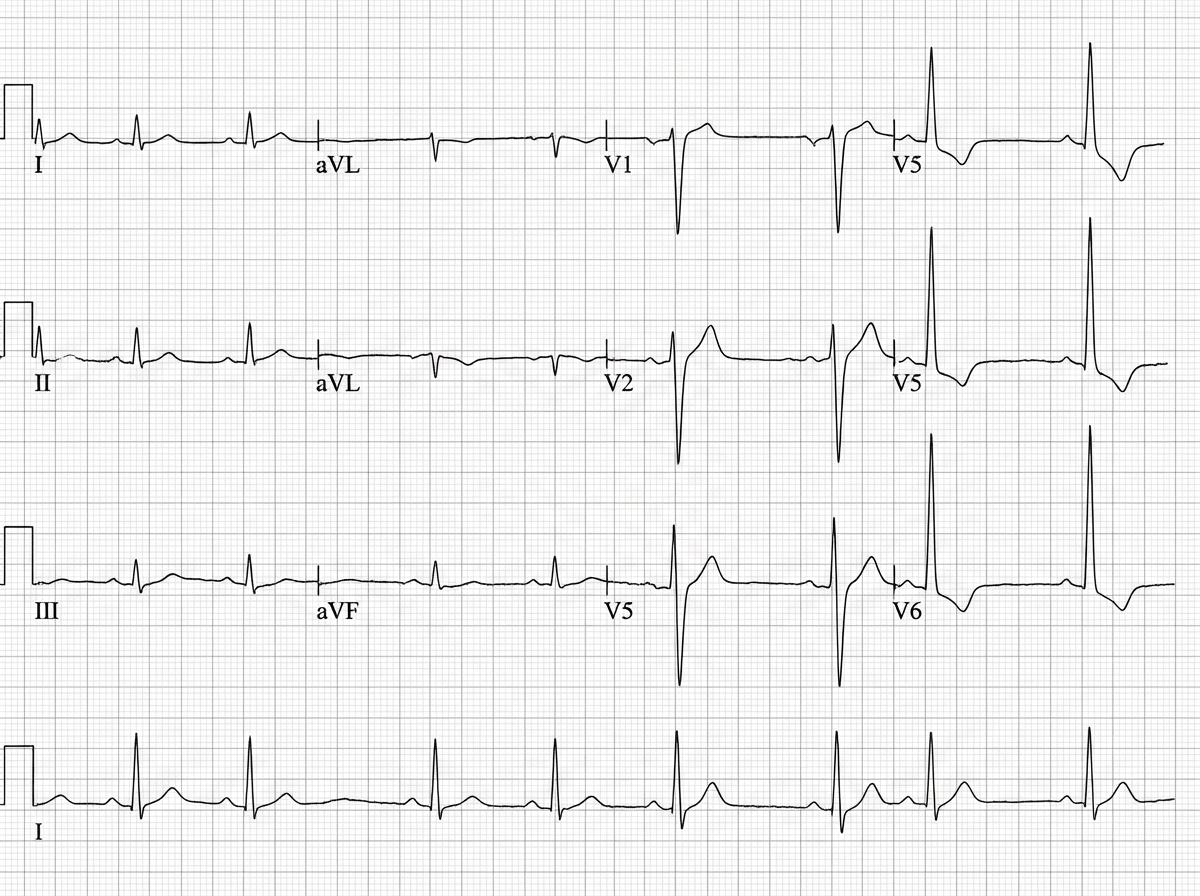
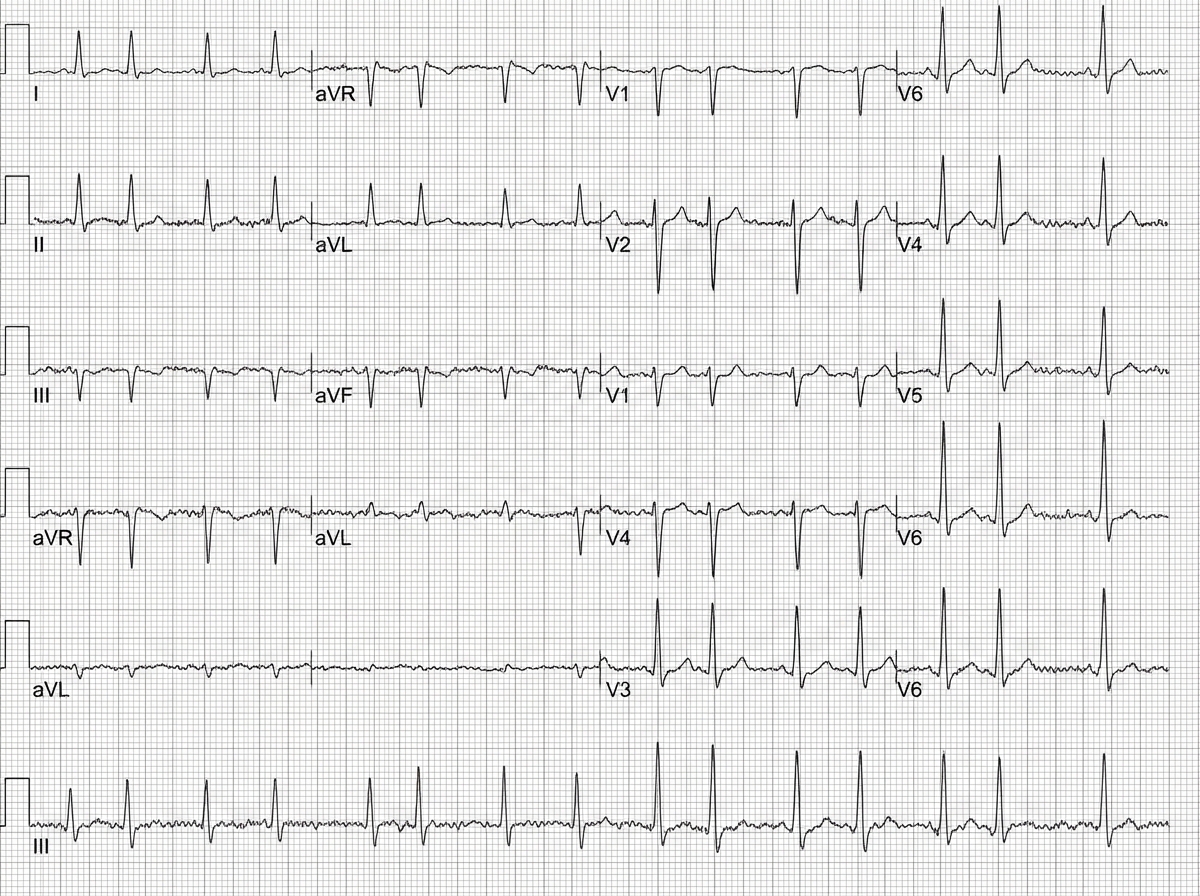
A 60-year-old hypertension patient presents with breathlessness. ECG was performed. What is the diagnosis? (Recent NEET Pattern 2016-17)
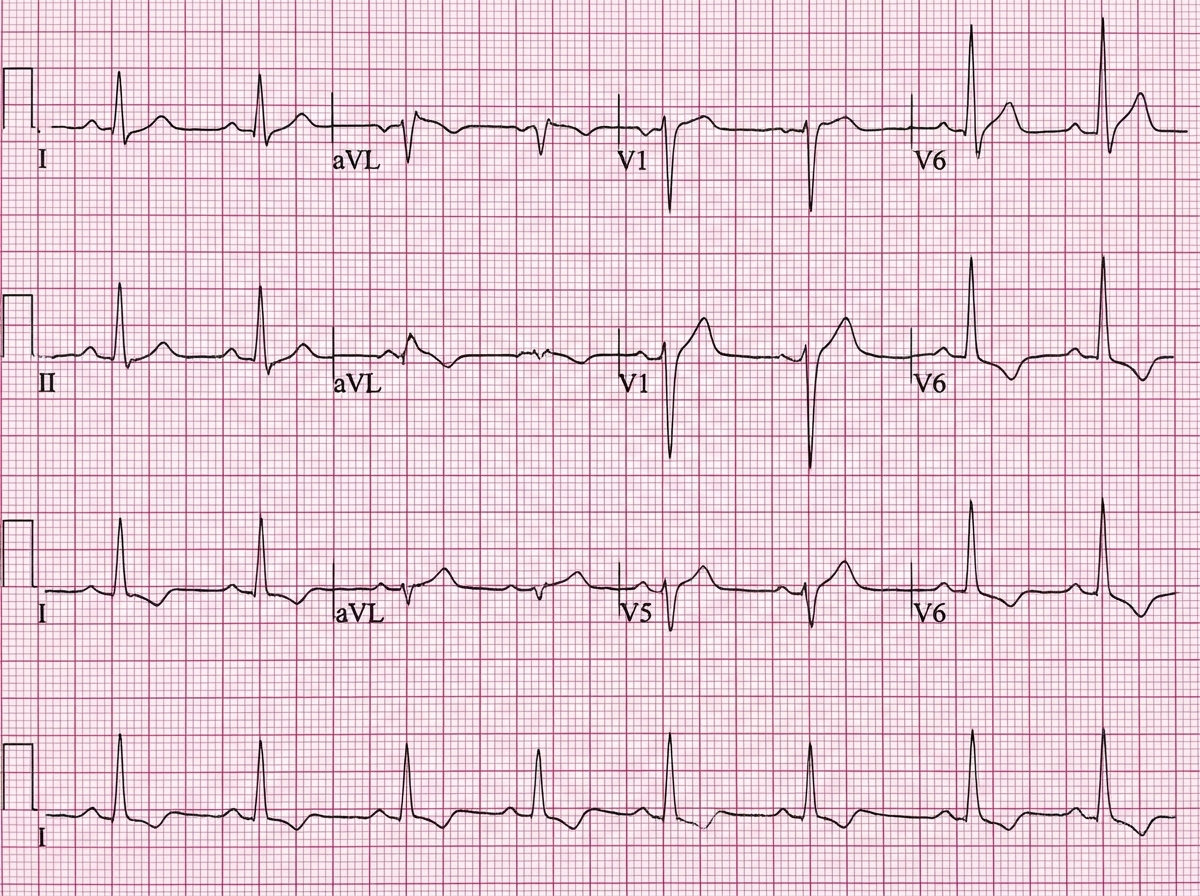
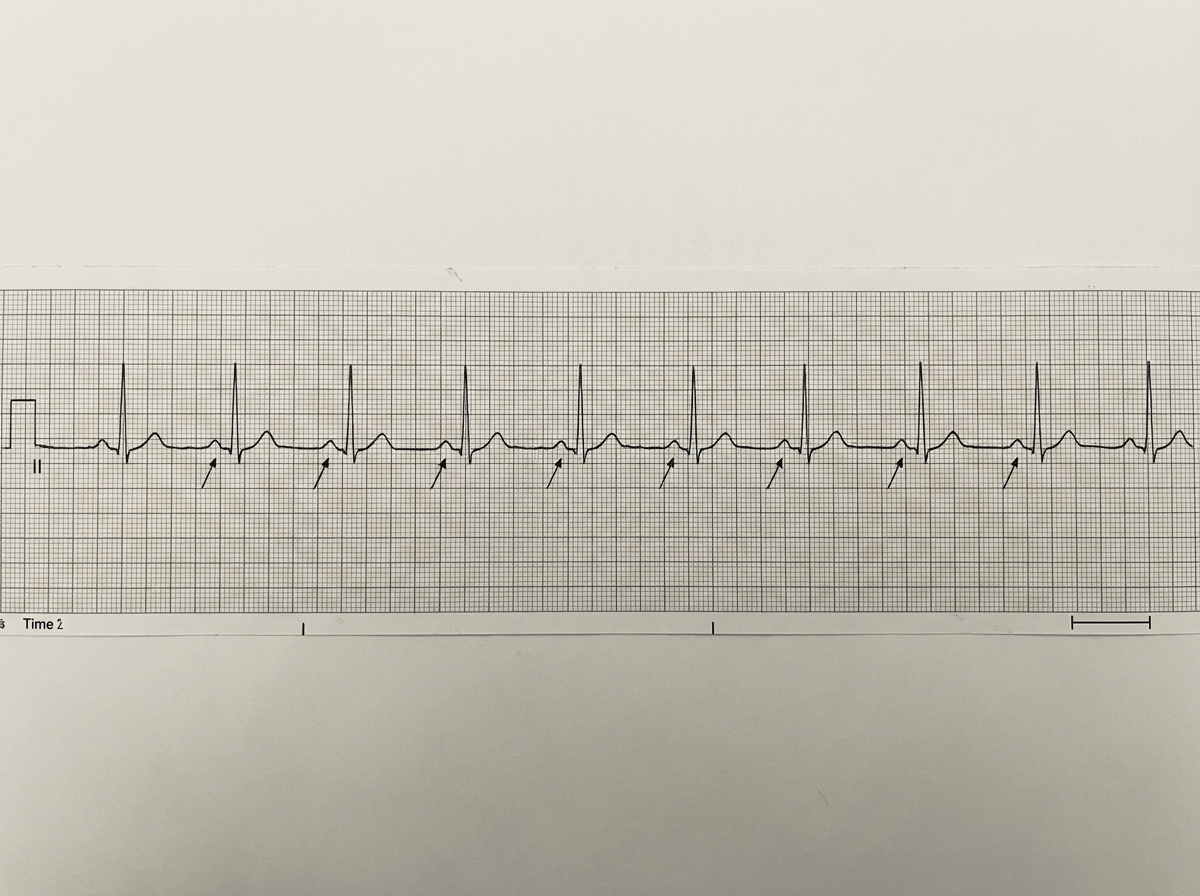
What does the following ECG show?
A marathon runner develops occasional missed beats. ECG shows:
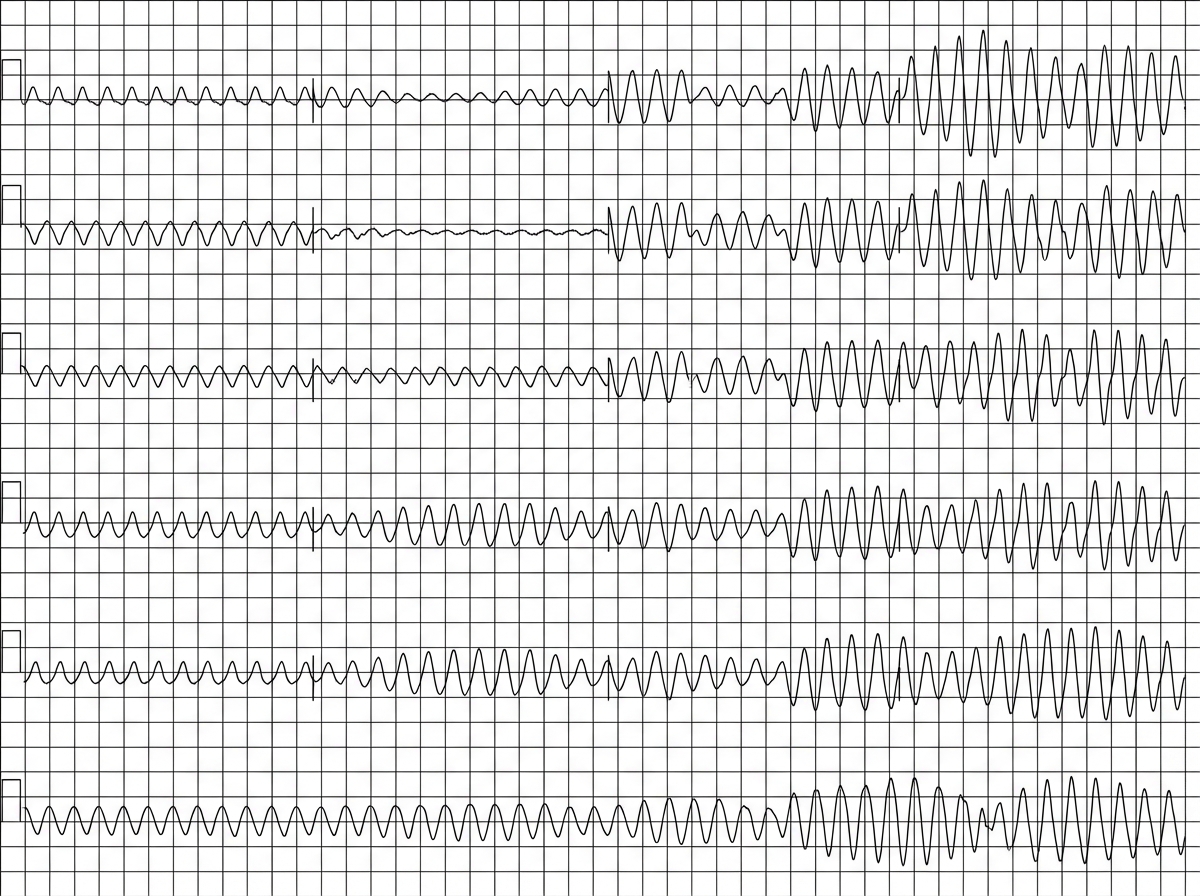
A 55-year-old woman with non-ischemic cardiomyopathy presents with palpitations. She is currently taking sotalol for rate control, and her most recent electrolytes showed hypokalemia (K+ 2.8 mEq/L). A preceding sinus-rhythm strip demonstrated a markedly prolonged QTc interval. ECG now shows:
A patient becomes pulseless and his BP crashes after myocardial infarction. Diagnosis is:
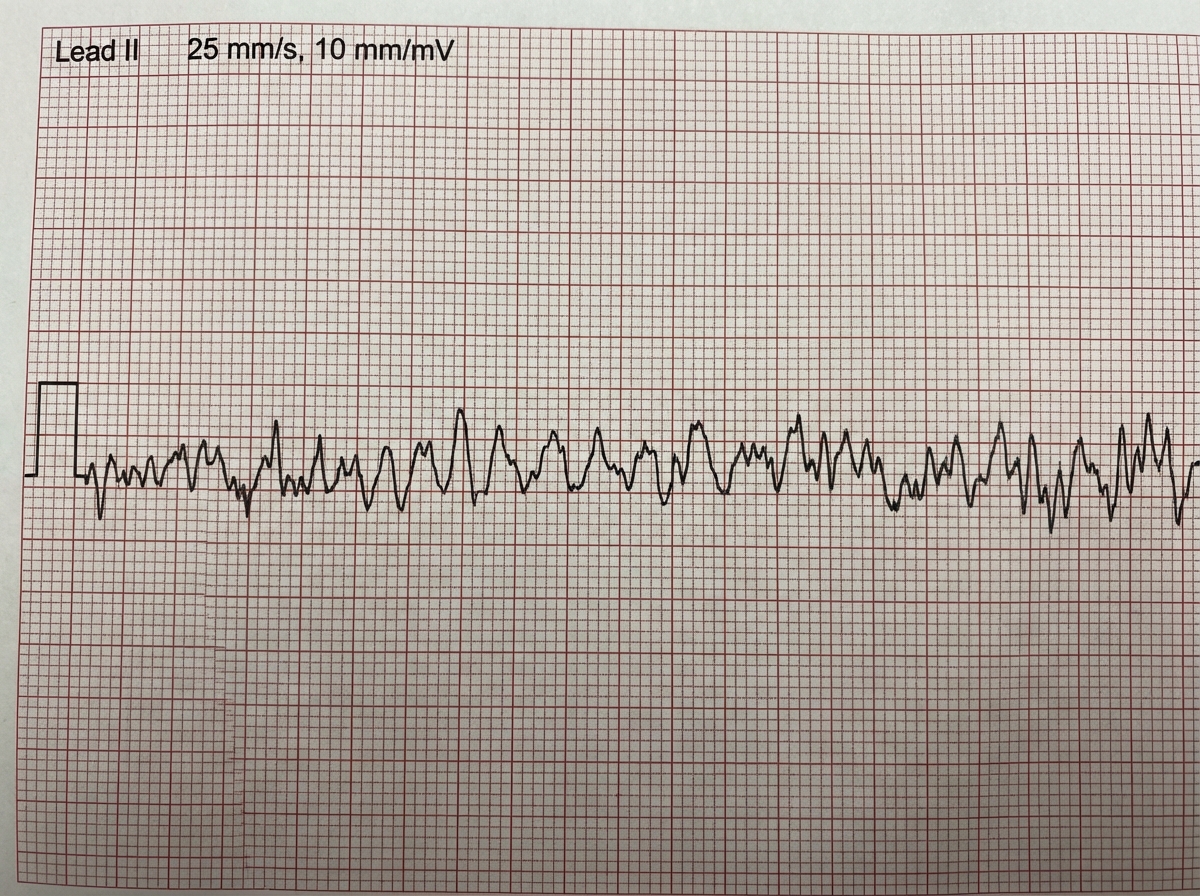
Identify the arrhythmia shown below:
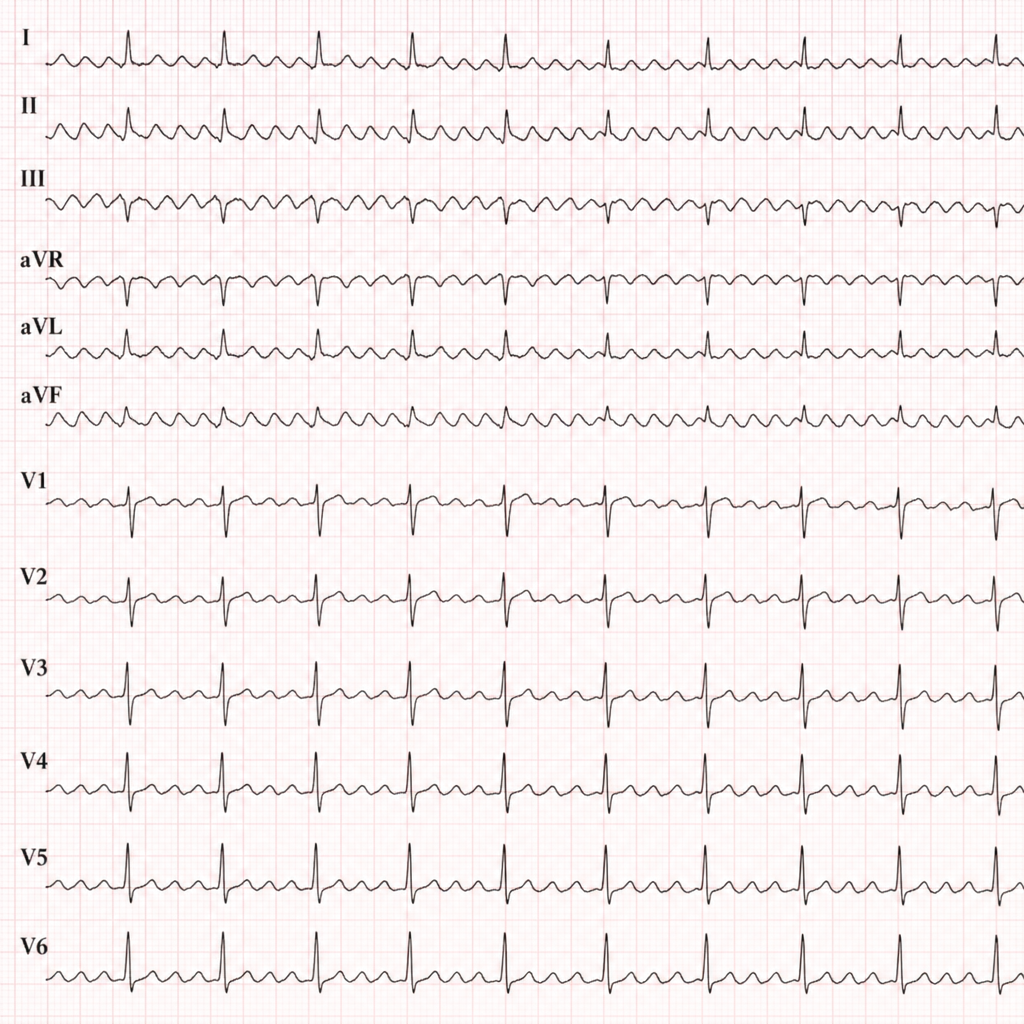
A 68 -year-old man presents with symptoms of alcohol withdrawal. ECG shows:
Comment on the diagnosis from the ECG shown below:
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app