
Cardiology — MCQs

On this page
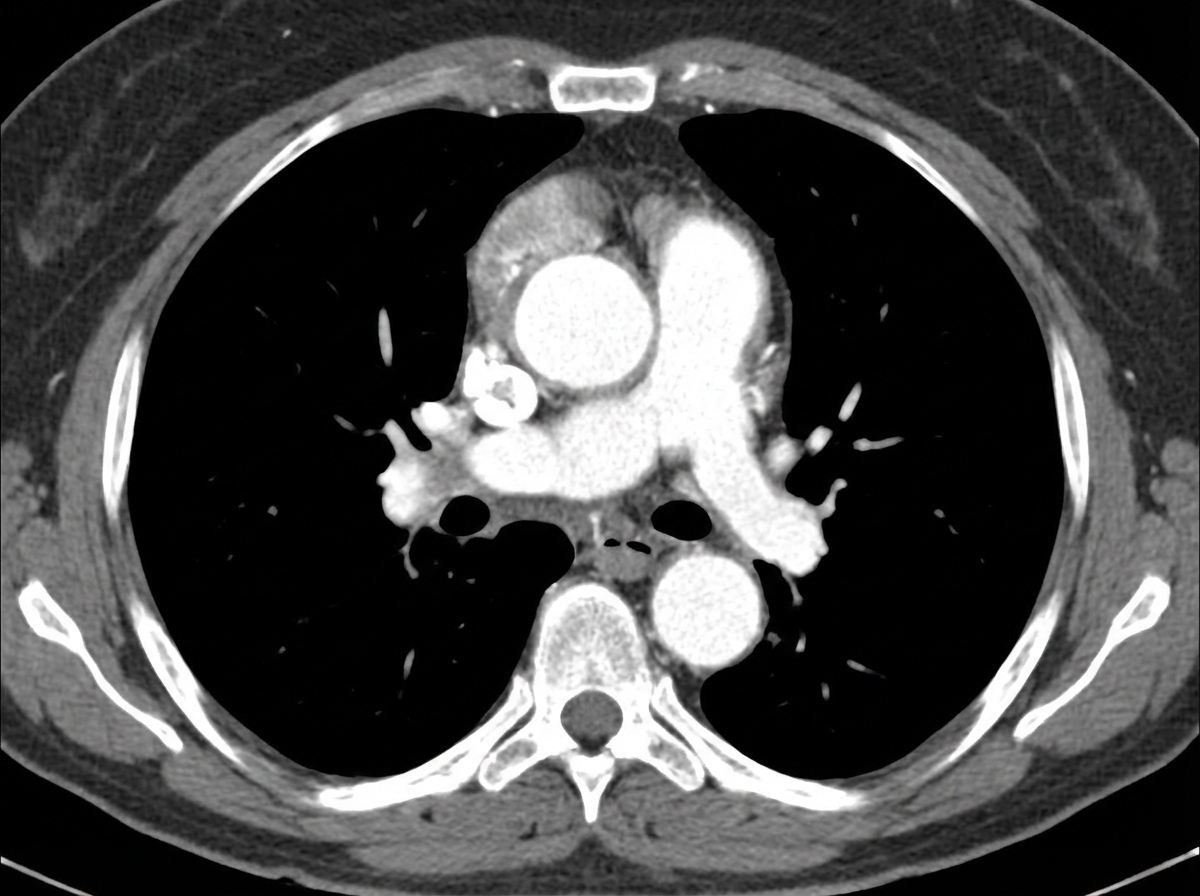
A 43-year-old man from Chile comes to the physician because of a 1-day history of upper back pain and difficulty swallowing. He has had pain in his shoulder and knee joints over the past 10 years. He is 190 cm (6 ft 3 in) tall and weighs 70.3 kg (155 lb); BMI is 19.4 kg/m2. His blood pressure is 142/86 mm Hg in the right arm and 130/70 mm Hg in the left arm. Physical examination shows a depression in the sternum and a grade 3/6 diastolic murmur at the right upper sternal border. A CT scan of the chest with contrast is shown. Which of the following is the most likely underlying cause of this patient's condition?
A 40-year-old man presents to the physician for a scheduled checkup. He was diagnosed with type 2 diabetes mellitus 5 years ago and has been taking his prescribed metformin daily, as prescribed. He also started exercising and has improved his diet. He has no particular complaints at the time. The patient has no other medical concerns and takes no medications. There is no family history of cardiovascular disease or diabetes. He does not smoke tobacco, drink alcohol, or use illicit drugs. Vitals are normal. There are no physical findings. His laboratory tests show: Serum glucose (fasting) 149 mg/dL Hemoglobin A1c 7.7 % Serum electrolytes Sodium 142 mEq/L Potassium 3.9 mEq/L Chloride 101 mEq/L Serum creatinine 0.8 mg/dL Blood urea nitrogen 9 mg/dL Urinalysis Glucose Negative Ketones Negative Leucocytes Negative Nitrite Negative Red blood cells (RBC) Negative Casts Negative Which of the following lipid profile abnormalities is most likely to be seen?
A 35-year-old woman presents with increased anxiety and a reeling sensation. Her complaint started 30 minutes ago with increased sweating and palpitations and is gradually worsening. On examination, the blood pressure was found to be 194/114 mm Hg. She had normal blood pressure at the local pharmacy 5 days ago. She currently works as an event manager and her job involves a lot of stress. The family history is significant for thyroid carcinoma in her father. Which of the following is most likely in this person?
A 69-year-old woman is brought to the emergency department because of fatigue and lethargy for 5 days. She has also had weakness and nausea for the last 3 days. She has sarcoidosis, major depressive disorder, and hypertension. She had a stroke 5 years ago. Current medications include aspirin, nifedipine, prednisolone, fluoxetine, and rosuvastatin, but she has not taken any of her medications for 7 days due to international travel. Her temperature is 36.1°C (96.9°F), pulse is 95/min, and blood pressure is 85/65 mm Hg. She is lethargic but oriented. Examination shows no other abnormalities. Her hemoglobin concentration is 13.4 g/dL and leukocyte count is 9,600/mm3. Both serum cortisol and ACTH levels are decreased. This patient is most likely to have which of the following additional laboratory abnormalities?
A 34-year-old G3P2103 with a past medical history of preeclampsia in her last pregnancy, HIV (CD4: 441/mm^3), and diabetes mellitus presents to her obstetrician for her first postpartum visit. She delivered her third child via C-section one week ago and reports that she is healing well from the surgery. She says that breastfeeding has been going well and that her baby has nearly regained his birth weight. The patient complains that she has been more tired than expected despite her efforts to sleep whenever her baby is napping. She relies on multiple iced coffees per day and likes to eat the ice after she finishes the drink. Her diet is otherwise unchanged, and she admits that she has not been getting outside to exercise as much as usual. Her home medications include metformin and her HAART regimen of dolutegravir, abacavir, and lamivudine. Her temperature is 98.9°F (37.2°C), blood pressure is 128/83 mmHg, pulse is 85/min, and respirations are 14/min. On physical exam, she is tired-appearing with conjunctival pallor. Given this patient's clinical presentation suggestive of iron deficiency anemia, which of the following complications is she most at risk of developing?
A 68-year-old man comes to the emergency department because of a 1-week history of difficulty breathing. He has had recurrent palpitations over the past 2 years. During this time, he has also had several episodes of anxiety despite no change in his daily life. He has occasional sharp chest pain localized to the left upper sternal border. He has no abdominal pain or leg swelling. Two years ago, he had streptococcal pharyngitis, which was promptly treated with a 10-day course of penicillin. He has never traveled outside of the country. His temperature is 36.5°C (97.7°F), pulse is 82/min, and blood pressure is 140/85 mm Hg. Physical examination shows a 3/6 holosystolic murmur that is loudest at the apex and radiates to the axilla with a mid-systolic click. Bilateral fine crackles are heard on lung auscultation. Which of the following is the most likely cause of this patient's symptoms?
A 43-year-old woman comes to the physician for an annual health maintenance examination. On questioning, she has had fatigue and headaches for the last month. A few weeks ago, she had to have her wedding ring resized because it had become too small for her finger. She has mild persistent asthma and anxiety disorder. She drinks 2–3 glasses of red wine per night and has smoked one pack of cigarettes daily for 16 years. She works a desk job in accounting and has recently been working long hours due to an upcoming company merger. Her father has a history of a pituitary adenoma. Current medications include alprazolam, a fluticasone inhaler, and an albuterol inhaler. She is 160 cm (5 ft 3 in) tall and weighs 81.6 kg (180 lb); her BMI is 32 kg/m2. Her temperature is 37.2°C (99°F), pulse is 92/min, and blood pressure is 132/80 mm Hg. Examination shows no abnormalities. Fasting laboratory studies show: Hemoglobin 13 g/dL Serum Na+ 135 mEq/L K+ 4.6 mEq/L Cl- 105 mEq/L HCO3- 22 mEq/L Urea nitrogen 17 mg/dL Glucose 160 mg/dL Creatinine 0.9 mg/dL Which of the following is the most likely underlying mechanism of this patient's hyperglycemia?
A 27-year-old woman comes to the physician because of a 1-year history of progressive shortness of breath. She is now unable to jog for more than 10 minutes without stopping to catch her breath. Cardiac examination shows a harsh systolic, crescendo-decrescendo murmur best heard at the lower left sternal border. The murmur increases in intensity when she moves from a squatting to a standing position and decreases when she clenches her fists. The lungs are clear to auscultation. Which of the following is the most likely cause of her condition?
A 27-year-old woman presents to her primary care physician with a chief complaint of pain in her hands, shoulders, and knees. She states that the pain has lasted for several months but seems to have worsened recently. Any activity such as opening jars, walking, or brushing her teeth is painful. The patient has a past medical history of a suicide attempt in college, constipation, anxiety, depression, and a sunburn associated with surfing which was treated with aloe vera gel. Her temperature is 99.5°F (37.5°C), blood pressure is 137/78 mmHg, pulse is 92/min, respirations are 14/min, and oxygen saturation is 98% on room air. Laboratory values are obtained and shown below. Hemoglobin: 9 g/dL Hematocrit: 33% Leukocyte count: 2,500/mm^3 with normal differential Platelet count: 107,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 102 mEq/L K+: 4.4 mEq/L HCO3-: 24 mEq/L BUN: 21 mg/dL Glucose: 90 mg/dL Creatinine: 1.0 mg/dL Ca2+: 10.2 mg/dL AST: 12 U/L ALT: 10 U/L Which of the following is the most likely to be found in this patient?
A previously healthy 46-year-old man comes to the physician for an 8-month history of headache that is more severe in the mornings. His blood pressure is 151/92 mm Hg. Examination shows enlargement of the nose, forehead, and jaw as well as the hands, fingers, and feet. Ophthalmologic examination shows impaired vision in the outer peripheral fields of both eyes. Laboratory studies show a serum glucose concentration of 225 mg/dL. Which of the following findings is most likely to confirm the diagnosis?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app