
Cardiology — MCQs

On this page
A 48-year-old woman presents to her family physician for evaluation of increasing shortness of breath. She returned from a trip to China 2 weeks ago and reports fever, myalgias, headaches, and a dry cough for the past week. Over the last 2 days, she has noticed increasingly severe shortness of breath. Her past medical history is non-contributory. The heart rate is 84/min, respiratory rate is 22/min, temperature is 38.0°C (100.4°F), and blood pressure is 120/80 mm Hg. A chest X-ray shows bilateral patchy infiltrates. Laboratory studies show leukopenia. After appropriate implementation of infection prevention and control measures, the patient is hospitalized. Which of the following is the most appropriate next step in management?
A 68-year-old, overweight gentleman with a 20-pack-year history of smoking presents to the primary care physician after noticing multiple blood-stained tissues after coughing attacks in the last month. His vital signs are within normal limits except for an O2 saturation of 93% on room air. He states that over the last 5 years his cough has continued to worsen and has never truly improved. He states that his shortness of breath has also worsened over this time period, as now he can barely make it up the flight of stairs in his home. In this patient, what is the most likely cause of his hemoptysis?
A 44-year-old woman presents to the outpatient clinic after she ran into a minor car accident. She says that she did not see the other car coming from the side and this is not the first time this has happened. When asked about any health issues she expresses concerns about whitish discharge dripping from both of her nipples that soils her blouse often. She is sexually active and has missed her periods for the last 3 months which she attributes to early signs of menopause. She denies nausea, vomiting, or recent weight gain. She currently does not take any medication. A visual field test reveals loss of bilateral temporal vision. Which of the following tests would best aid in diagnosing this patient’s condition?
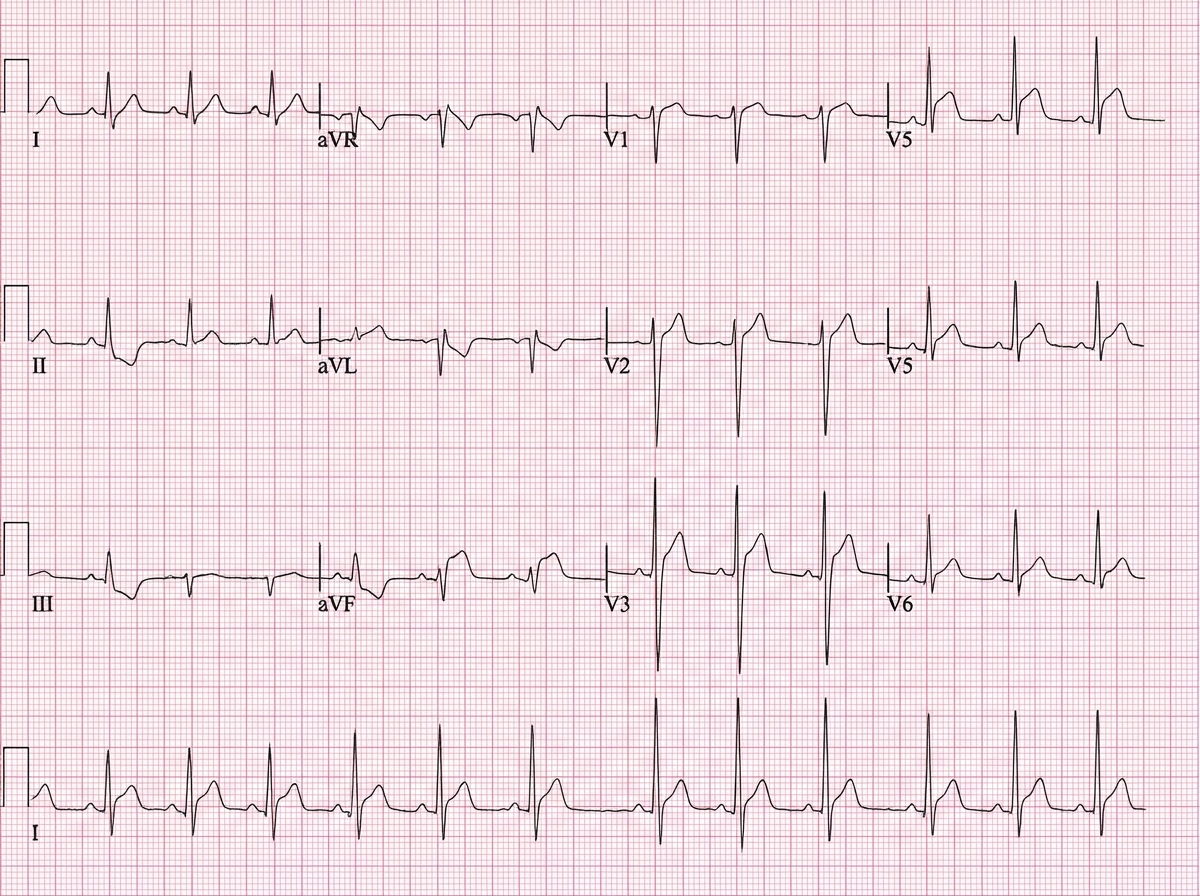
An otherwise healthy 31-year-old man presents to the emergency department with a several-day history of sharp, central chest pain, which is constant and unrelated to exertion. The pain gets worse on lying down and decreases with sitting forward. He has smoked 10–15 cigarettes daily for the past 7 years. His blood pressure is 120/50 mm Hg, the pulse is 92/min, and the temperature is 37.1°C (98.7°F). On physical examination, a scratching sound is heard at end-expiration with the patient leaning forward. ECG is shown in the image. Serum troponin is mildly elevated. Which of the following is the most likely diagnosis?
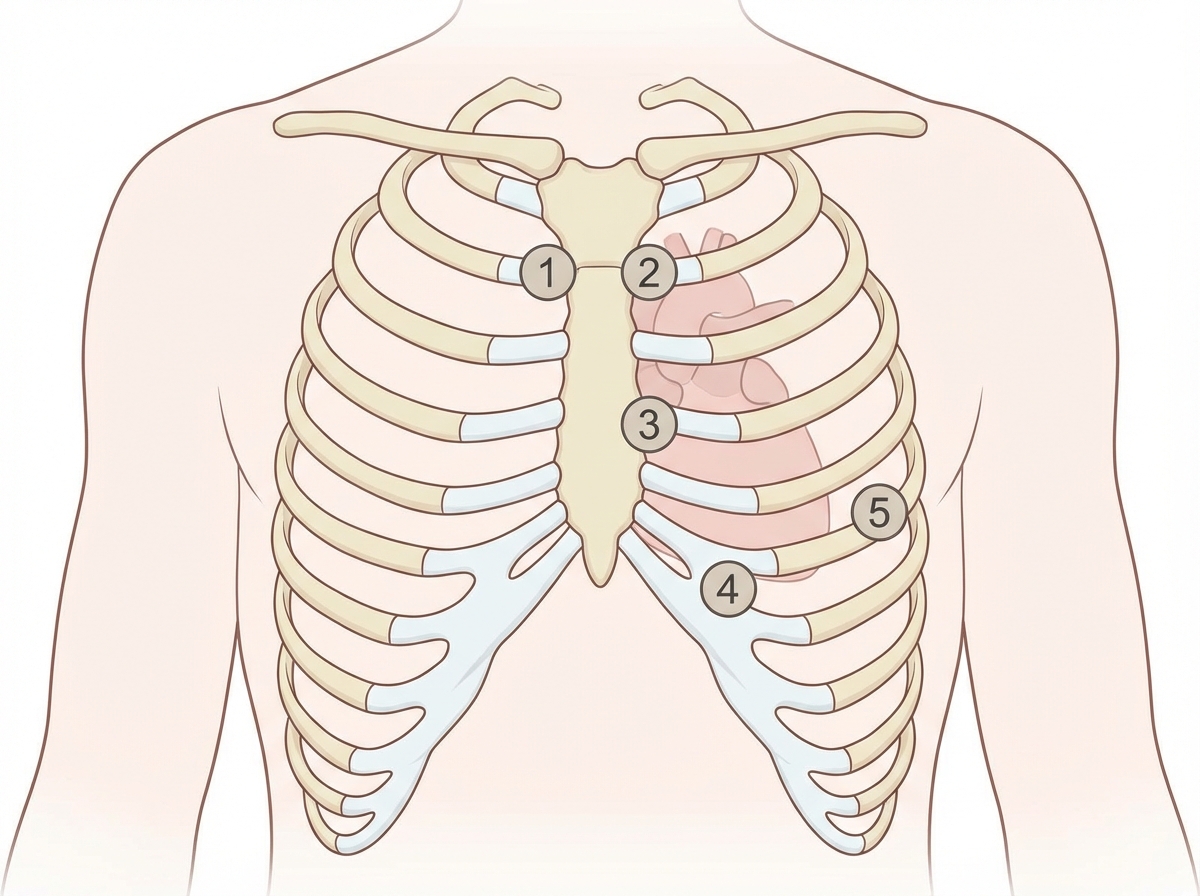
A 27-year-old woman, who recently immigrated from Bangladesh, presents to her primary care physician to discuss birth control. During a review of her past medical history, she reports that as a child she had a recurrent sore throat and fever followed by swollen and aching hip and knee joints. These symptoms returned every season and were never treated but went away on their own only to return with the next typhoon season. When asked about any current complaints, the patient says that she sometimes has shortness of breath and palpitations that do not last long. A physical exam is performed. In which of the auscultation sites will a murmur most likely be heard in this patient?
A 60-year-old man comes to the physician for a routine health maintenance examination. Over the past year, he has had problems initiating urination and the sensation of incomplete bladder emptying. He has a history of hypertension and hypercholesterolemia. He has smoked one pack of cigarettes daily for the past 40 years. He does not drink alcohol. His medications include lisinopril, atorvastatin, and daily aspirin. Vital signs are within normal limits. Physical examination shows a pulsatile abdominal mass at the level of the umbilicus and a bruit on auscultation. Digital rectal examination shows a symmetrically enlarged, smooth, firm, nontender prostate with rubbery texture. Laboratory studies are within normal limits. Which of the following is the most appropriate next step in management?
A 48-year-old man is brought to the emergency department by his neighbor, who found him lying unconscious at the door of his house. The patient lives alone and no further history is available. On physical examination, his temperature is 37.2ºC (98.9ºF), pulse rate is 114/min, blood pressure is 116/78 mm Hg, and respiratory rate is 22/min. His Glasgow Coma Scale score is 7 and the patient is intubated. A stat serum osmolality is reported at 260 mmol/kg. Based on the provided information, which of the following conditions is most likely present in this patient?
A 72-year-old man presents to his primary care physician for a general checkup. The patient works as a farmer and has no concerns about his health. He has a past medical history of hypertension and obesity. His current medications include lisinopril and metoprolol. His temperature is 99.5°F (37.5°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for a murmur after S2 over the left sternal border. The patient demonstrates a stable gait and 5/5 strength in his upper and lower extremities. Which of the following is another possible finding in this patient?
A 52-year-old man presents to a medical clinic to establish care. He has no known chronic illnesses but has not seen a physician in over 20 years. He generally feels well but occasionally has shortness of breath when he jogs and exercises. He smokes 2-5 cigarettes per day and uses IV heroin “now and then.” Physical exam is unremarkable. ECG shows prominent QRS voltage and left axis deviation. Trans-thoracic echocardiogram shows mild concentric left ventricular hypertrophy but is otherwise normal. Which of the following is the most likely etiology of the echocardiogram findings?
A 34-year-old woman comes to the physician because of a 3-month history of fatigue and a 4.5-kg (10-lb) weight loss despite eating more than usual. Her pulse is 115/min and blood pressure is 140/60 mm Hg. Physical examination shows warm, moist skin, and a diffuse, non-tender swelling over the anterior neck. Ophthalmologic examination shows swelling of the eyelids and proptosis bilaterally. Which of the following is the most likely cause of this patient's symptoms?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app